

Introduction
Primary eye care is a vital component in primary health care and includes the promotion of eye health care, the prevention and treatment of conditions that may lead to visual loss, as well as the rehabilitation of those who are already blind. The aim of primary eye care is to change the pattern of eye care services, currently often limited to the central hospitals and eye units in the cities, to countrywide blindness prevention programmes.
Primary eye care is the primary health care approach to the prevention of blindness and it should be an integral part of primary health care. Primary health care is defined as essential health care based on methods and technology that are practical and scientifically sound, as well as socially acceptable; accessible to the community, affordable for the community with good community participation.1
In most developing countries avoidable blindness constitutes a major public health problem. There are distinct, closely related components in the primary health care approach to blindness prevention. Only one of the components requires interaction between the sick individual and medical personnel.
In many developing countries there are insufficient trained staff, and eye care services have to be given to widely and often sparsely scattered populations.2 An ophthalmologist in such a setting becomes overwhelmed with the demands that require his or her attention. Reviewing activities at the end of the year reveals that very few of the diseases that cause over 70% of blindness have been significantly addressed.3 Most of the blindness we encounter is avoidable. Cataract is responsible for nearly 50% of blindness throughout the world.4 In fact most of the cases that occupy the ophthalmologist's time can be delegated to others if they are adequately trained and equipped. We began an exercise to prepare suitable personnel. Our aims were as follows:
Train at least one integrated eye worker and staff in every health care institution.
Staff an ophthalmic clinical officer or an ophthalmic nurse at each General/ District Hospital.
Teach each traditional birth attendant (TBA), community health worker (CHW), community based rehabilitation worker (CBRW) to understand how to prevent blindness.
We are now interacting with the traditional healers to collaborate with them in the prevention of blindness. We also support these groups of eye workers through:
Regular visits to their centres
Taking referrals
Supplying essential eye medications
General supplies
Continuing education.
As a result of this exercise we were able to increase our cataract surgical rate threefold.
Categories of Eye Care Workers
Eye care staff can be grouped into three main categories:2
-
Full time eye care workers.
- Ophthalmologists
- Ophthalmic clinical officers
- Ophthalmic nurses
- Optical technicians
-
Integrated eye care workers. All health workers of any type must be involved in integrated eye care services and eye care as part of their day-to-day routine.
- General practitioners
- Clinical officers
- Nurses
- Midwives
- Environmental health technicians
-
Community eye care workers. These are people who, in the course of their normal work, have close contact with the community, especially at village level, including CHWs, TBAs, CBR volunteers and traditional healers. These colleagues, by use of appropriate knowledge, can be instrumental in the prevention of blindness. Other nonmedical personnel whose contribution and participation can enhance the blindness prevention activities include:
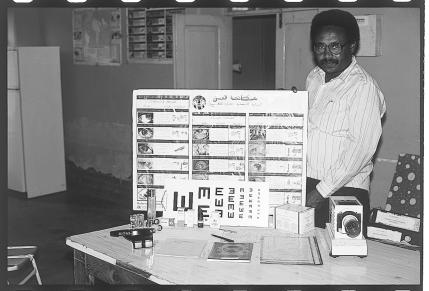 Mr Bashir El-Tayeb Mohd., senior ophthalmic medical assistant, with teaching materials used in training community health workers. Kassala State, SudanPhoto: Murray McGavin
Mr Bashir El-Tayeb Mohd., senior ophthalmic medical assistant, with teaching materials used in training community health workers. Kassala State, SudanPhoto: Murray McGavin- School teachers
- Church/religious leaders
- Agriculture extension officers
- Water department officers
- Headmen
- Social welfare officers

Job Description
Primary eye care activities are as follows:
-
Creating awareness (promotive). This is the strengthening of community awareness and co-operation to promote health within the family unit. Appropriate information is disseminated to as many people in the community as possible. Current traditional health education methods carried out in clinics and health centres are not appropriate, hence the impact of such methods are negligible. People from within the community are very effective in creating awareness. In using the appreciative inquiry method we ask the question, “In this community what are the existing communication lines that we can use?”. The answer is, there are several. These include:
- The ophthalmologist who passes the information on to the trained health personnel.
-
Trained health personnel who use this information to train others, for example:
-
Community health workers: These include community health workers or primary health workers; traditional birth attendants (TBA); community baseddistributors(CBD); and, recently, community based rehabilitation workers (CBRW). These are people chosen by their respective communities to look into the affairs of the community's health. They know how to present the information given to them in a language the community will understand and accept.
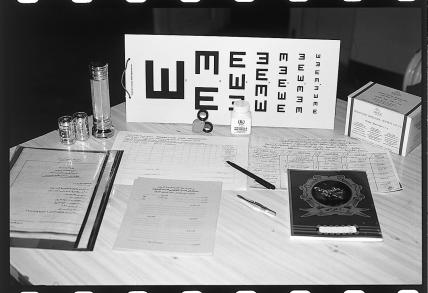 Equipment given to community health workers after training. Kassala State, SudanPhoto: Murray McGavin
Equipment given to community health workers after training. Kassala State, SudanPhoto: Murray McGavin - Community leaders: These include village headmen, church leaders and other influential people in the community.
- Administrative authorities: These are local government officials and departmental managers.
- School teachers: Professionals who will make eye health part of the school curriculum and thus create a new generation of citizens who know about blindness and its prevention.
- Traditional healers: These are health care providers who are accessible in their communities. Given the correct information, these people will provide a potential cadre of primary eye care workers.
The information given to pass on includes: -
- The burden blindness brings to individuals who are themselves blind, and on the family at home and on the community as a whole.
- The major blinding diseases which are common in the area and how blindness can be avoided.
- Understanding of basic first aid skills in case of accidents and treatment of the common eye diseases.
- Offering guidance to the community on how to arrange transportation and reach the health centre where more help can be given.
-
Prevention: This includes stimulation of individuals and their community to participate in activities in blindness prevention; social and community development that promotes health through changes in behaviour and environment and leads to the reduction or elimination of factors contributing to ocular disease. Examples of activities are as follows:
- Provision of adequate, safe water supplies; personal hygiene.
- Construction, use and maintenance of pit latrines and refuse pits; environmental hygiene.
- Growing and consumption of foods rich in vitamin A; nutrition.
- Recognition and appropriate care of individuals at risk of blinding diseases; for example, adequate feeding and rehydration of children with severe measles, malnutrition or diarrhoea.
- Protection of eyes against injuries.
- Immunisation against measles.
- Screening of antenatal mothers for sexually transmitted diseases.
Most of these can be done by the environmental health technician or health inspector, community health nurses, community health volunteers, school teachers, agricultural extension officers, nutritionists, road traffic inspectors, and other community members. Satisfied former cataract patients will respond to a request to direct others to the clinics for appropriate treatment. The key roles of the trained eye health personnel involves training and support.
-
Curative activities: This involves delivery of eye care to all individuals with potentially blinding disorders in the communities. For example:
- First aid treatment and/or timely referral of patients with injuries.
- Identification and treatment/referral of common eye diseases.
- Identification and referral of patients with potentially blinding diseases for appropriate management.
- Identification and referral of curable blinding diseases like cataracts.
These activities are mostly carried out by community health volunteers who refer to the trained health personnel who eventually hand the patients over to the trained eye workers.
Rehabilitation activities: What happens to those who are incurably blind? Do we merely sympathise with them and their families? Since primary eye care is mainly concerned with the community level, the issue of rehabilitation becomes very important. Clients are assured that they are not completely useless. With training, skills can be acquired and they can be functional and not have to rely totally on others. Here the CBR volunteers, as well as all the other volunteer workers, are very important. All trained health personnel, school teachers, social workers can connect these incurably blind to rehabilitation programmes that exist in the area (Table 1).

Table 1.
Primary Eye Care Activities
| Activity | What? | Where? | Who? |
|---|---|---|---|
| Awareness creation | Teaching about blindness, its effects and its causes | Community, Schools, Health Centres, Hospitals |
Community health workers, Traditional healers, School teachers, Pupils, Trained health workers, Community leaders, Media |
| Preventive activities | Immunisation Water and Sanitation Nutrition Prevention of injuries Antenatal screening Eye prophylaxis for the new born |
Community, Health Centres, Hospitals |
Community health workers, Traditional healers, Parents, Environmental health technicians, Public health nurses, Midwives, Clinical officers, Medical officers |
| Clinical | First Aid management of injuries Recognition and management of common eye diseases Recognition and management/referral of potential blinding diseases Recognition and management referral of curable eye diseases — e.g., cataract |
Community, Health Centres, Hospitals |
Community health workers, Traditional healers, Nurses, Clinical officers, Midwives, Medical officers, Ophthalmic nurses and Ophthalmic clinical officers |
| Rehabilitation | Identification of the incurably blind directing them to an appropriate rehabilitation programme | Community, Health Centres, Hospitals |
Parents, Teachers, Community health workers, Trained medical personnel, Community based rehabilitation workers, Social workers, Community leaders |
Conclusion
To have a successful primary eye care programme, there needs to be coordinated teamwork. There should be regular interaction between the full time eye workers, the integrated eye workers and the volunteer eye workers. The complementary nature of the team needs to be understood and appreciated.5 Task oriented training of all team members should be based on the skills that they need to acquire and in which competence is necessary.
References
- 1.Chana HS. Eye Care Programmes in Developing Countries. Nairobi: Majestic Printing Works; 1989. Primary Eye Care; p. 58. [Google Scholar]
- 2.Taylor J. Appropriate methods and resources for third world ophthalmology. Duane's Clinical Ophthalmology. 1989;Vol. 5:1–2. Chapter 58. [Google Scholar]
- 3.WHO. Fact Sheet No. 142–147. February 1997.
- 4.Foster A Eye Diseases in the Tropics. CBM Fact Sheet. July 1995. 5. [Google Scholar]
- 5.1990. Management of Cataract in Primary Health Care Services; p. 26. WHO/Geneva. [Google Scholar]