

Abstract
Methods: Lateral neck radiograph was performed on 35 children referred consecutively to a university paediatric chest clinic for suspected OSA secondary to tonsillar hypertrophy. The tonsil size was determined by measuring the TP ratio on the radiographs. The severity of OSA was assessed by overnight polysomnography.
Results: A total of 24 boys and 11 girls (median age 6.2 years) were studied. All presented with symptoms of OSA, and tonsillar hypertrophy was detected on clinical examination. The median apnoea–hypopnoea index (AHI) was 16.93 (interquartile range: 8.41 to 28.29). The median TP ratio was 0.76 (interquartile range: 0.65 to 0.80). AHI was positively correlated with the TP ratio. The clinical tonsil size did not correlate with the AHI or the TP ratio. Using a TP ratio of 0.479, the sensitivity and specificity in predicting cases with moderate/severe OSA (AHI >10) were 95.8% and 81.8% respectively, while the positive and negative predictive values were 92.0% and 90.0% respectively.
Conclusions: Results show that in a population of children with OSA, tonsillar hypertrophy as assessed by lateral neck radiograph correlates positively with the severity of obstructive sleep apnoea. The TP ratio has high sensitivity and specificity in predicting those with moderate/severe disease and this feature may be used as a clinical screening method in prioritising patients with OSA for further assessment.
Full Text
The Full Text of this article is available as a PDF (88.6 KB).
Figure 1 .
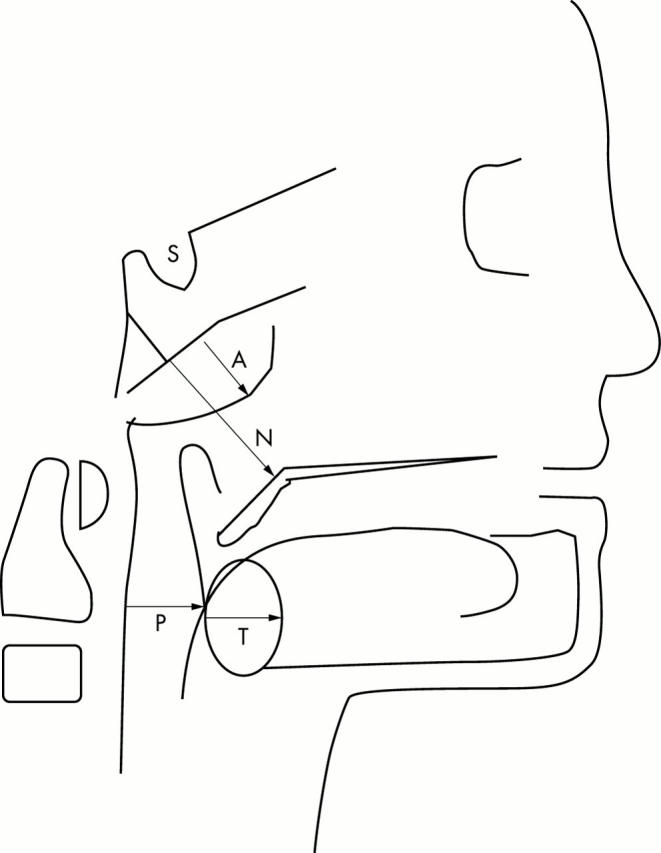
Graphic description of measurements of a lateral cephalography. A, adenoid; N, nasopharyngeal measurement; P, pharyngeal measurement; S, sella turcica; T, tonsil. A and T are measured as a perpendicular distance at their maximum convexity. T/P is the ratio of the width of the tonsil to the depth of the pharyngeal space.
Figure 2 .

Frequency of presenting clinical features of OSA in the subjects (n = 35).
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ahlqvist-Rastad J., Hultcrantz E., Svanholm H. Children with tonsillar obstruction: indications for and efficacy of tonsillectomy. Acta Paediatr Scand. 1988 Nov;77(6):831–835. doi: 10.1111/j.1651-2227.1988.tb10764.x. [DOI] [PubMed] [Google Scholar]
- Ali N. J., Pitson D. J., Stradling J. R. Snoring, sleep disturbance, and behaviour in 4-5 year olds. Arch Dis Child. 1993 Mar;68(3):360–366. doi: 10.1136/adc.68.3.360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bennett J. A., Kinnear W. J. Sleep on the cheap: the role of overnight oximetry in the diagnosis of sleep apnoea hypopnoea syndrome. Thorax. 1999 Nov;54(11):958–959. doi: 10.1136/thx.54.11.958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brodsky L. Modern assessment of tonsils and adenoids. Pediatr Clin North Am. 1989 Dec;36(6):1551–1569. doi: 10.1016/s0031-3955(16)36806-7. [DOI] [PubMed] [Google Scholar]
- Brooks L. J., Stephens B. M., Bacevice A. M. Adenoid size is related to severity but not the number of episodes of obstructive apnea in children. J Pediatr. 1998 Apr;132(4):682–686. doi: 10.1016/s0022-3476(98)70360-9. [DOI] [PubMed] [Google Scholar]
- Brouillette R. T., Fernbach S. K., Hunt C. E. Obstructive sleep apnea in infants and children. J Pediatr. 1982 Jan;100(1):31–40. doi: 10.1016/s0022-3476(82)80231-x. [DOI] [PubMed] [Google Scholar]
- Brouillette R. T., Manoukian J. J., Ducharme F. M., Oudjhane K., Earle L. G., Ladan S., Morielli A. Efficacy of fluticasone nasal spray for pediatric obstructive sleep apnea. J Pediatr. 2001 Jun;138(6):838–844. doi: 10.1067/mpd.2001.114474. [DOI] [PubMed] [Google Scholar]
- Corbo G. M., Fuciarelli F., Foresi A., De Benedetto F. Snoring in children: association with respiratory symptoms and passive smoking. BMJ. 1989 Dec 16;299(6714):1491–1494. doi: 10.1136/bmj.299.6714.1491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Croft C. B., Brockbank M. J., Wright A., Swanston A. R. Obstructive sleep apnoea in children undergoing routine tonsillectomy and adenoidectomy. Clin Otolaryngol Allied Sci. 1990 Aug;15(4):307–314. doi: 10.1111/j.1365-2273.1990.tb00474.x. [DOI] [PubMed] [Google Scholar]
- Frank Y., Kravath R. E., Pollak C. P., Weitzman E. D. Obstructive sleep apnea and its therapy: clinical and polysomnographic manifestations. Pediatrics. 1983 May;71(5):737–742. [PubMed] [Google Scholar]
- Leach J., Olson J., Hermann J., Manning S. Polysomnographic and clinical findings in children with obstructive sleep apnea. Arch Otolaryngol Head Neck Surg. 1992 Jul;118(7):741–744. doi: 10.1001/archotol.1992.01880070071013. [DOI] [PubMed] [Google Scholar]
- Metz C. E. Basic principles of ROC analysis. Semin Nucl Med. 1978 Oct;8(4):283–298. doi: 10.1016/s0001-2998(78)80014-2. [DOI] [PubMed] [Google Scholar]
- Shintani T., Asakura K., Kataura A. Adenotonsillar hypertrophy and skeletal morphology of children with obstructive sleep apnea syndrome. Acta Otolaryngol Suppl. 1996;523:222–224. [PubMed] [Google Scholar]
- Sofer S., Weinhouse E., Tal A., Wanderman K. L., Margulis G., Leiberman A., Gueron M. Cor pulmonale due to adenoidal or tonsillar hypertrophy or both in children. Noninvasive diagnosis and follow-up. Chest. 1988 Jan;93(1):119–122. doi: 10.1378/chest.93.1.119. [DOI] [PubMed] [Google Scholar]