

Full Text
The Full Text of this article is available as a PDF (133.3 KB).
Figure 1.
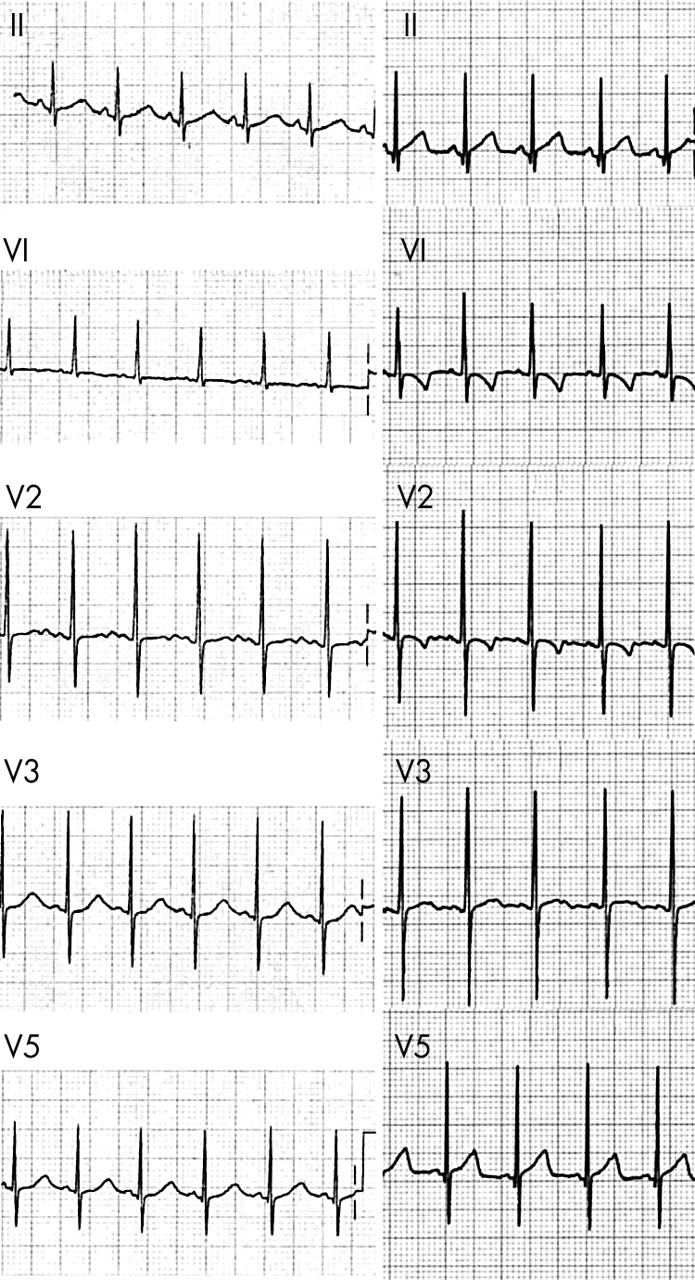
Extracts from the surface electrocardiogram. Left: The day after the cardiac arrest, the T-wave has a late onset and is broad, the QT is measured at a minimum of 0.32 seconds, R-R interval 0.44 seconds, giving a QTc of 0.48 seconds. On some beats the end of the T-wave is less clear, with a long gentle slope into the p-wave such that the true QTc may be a little longer. Right: At 3 months of age the 12 lead ECG is normal. The T-wave is not suspicious for long QT syndrome, and the QT is approximately 0.28 seconds, R-R interval 0.49 seconds, giving a QTc of 0.40 seconds. No features suggest Brugada syndrome.
Figure 2.

Sequence analysis of SCN5A ex20 using patient DNA. (A) The sequence reveals heterozygosity for guanine to adenine (G→A) nucleotide change (arrow) at the second position of codon 1193, which predicts a substitution of arginine by glutamine (R1193Q). (B) AciI restriction enzyme analysis of SCN5A exon 20 in the family members (lanes 1–3) and controls (lanes 4–7). The loss of an AciI site creates fragment sizes of 235bp and 181bp that are visible in the affected child and the maternal side of the family; whereas no 235bp fragments were observed in the paternal side of the family or in 90 control subjects.