

Abstract
Aim: To evaluate the changes in the osmolality of expressed breast milk (EBM) after the addition of seven additives and four proprietary fortifiers commonly used during neonatal intensive care.
Methods: The osmolality of 5 ml EBM was measured with increasing doses of 6% NaCl, caffeine, sodium ironedetate, folic acid, and multivitamin drops. Sodium acid phosphate and chloral hydrate were added to 8 ml EBM, and the fortifiers were added to standard volumes of EBM. Dose-effect curves were plotted, and the volume of milk that must be added to the above additives to maintain osmolality below 400 mOsm/kg was calculated.
Results: The osmolality of the pure additives ranged from 242 to 951 mOsm/kg. There was a significant increase in the osmolality of EBM with increasing doses of all additives except caffeine. The osmolality of EBM with many additives in clinically used dosages potentially exceeded 400 mOsm/kg. The greatest increase occurred with sodium ironedetate syrup, where the osmolality of EBM increased to 951.57 (25.36) mOsm/kg. Proprietary fortifiers increased the osmolality of EBM to a maximum of 395 mOsm/kg.
Conclusion: Routine additives can significantly increase the osmolality of EBM to levels that exceed current guidelines for premature infant feeding. A simple guide for clinical use is presented, which indicates the amount of milk required as diluent if hyperosmolality is to be avoided.
Full Text
The Full Text of this article is available as a PDF (136.3 KB).
Figure 1.
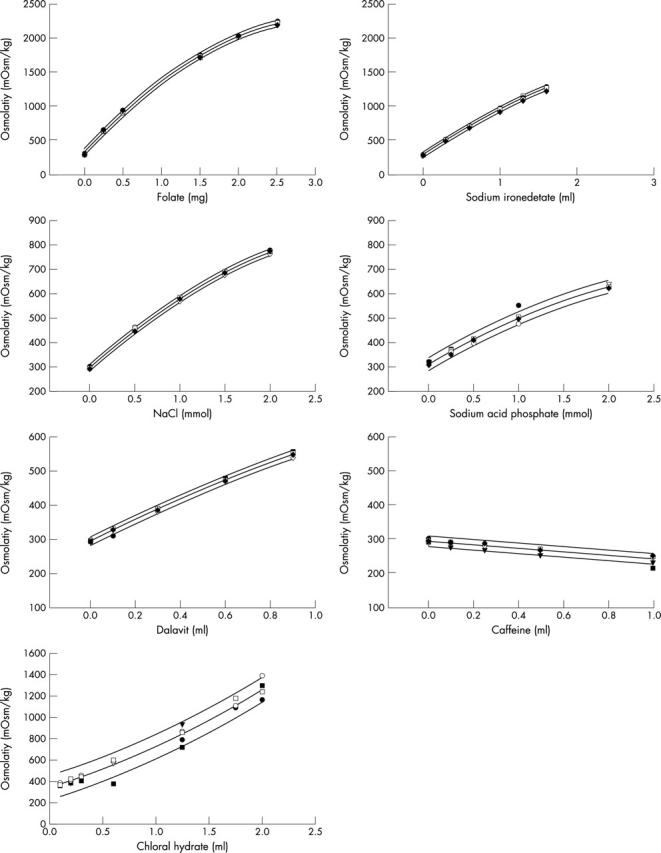
Osmolality of expressed breast milk with increasing doses of nutritional additives showing least squares linear regression and 95% confidence intervals.
Figure 2.
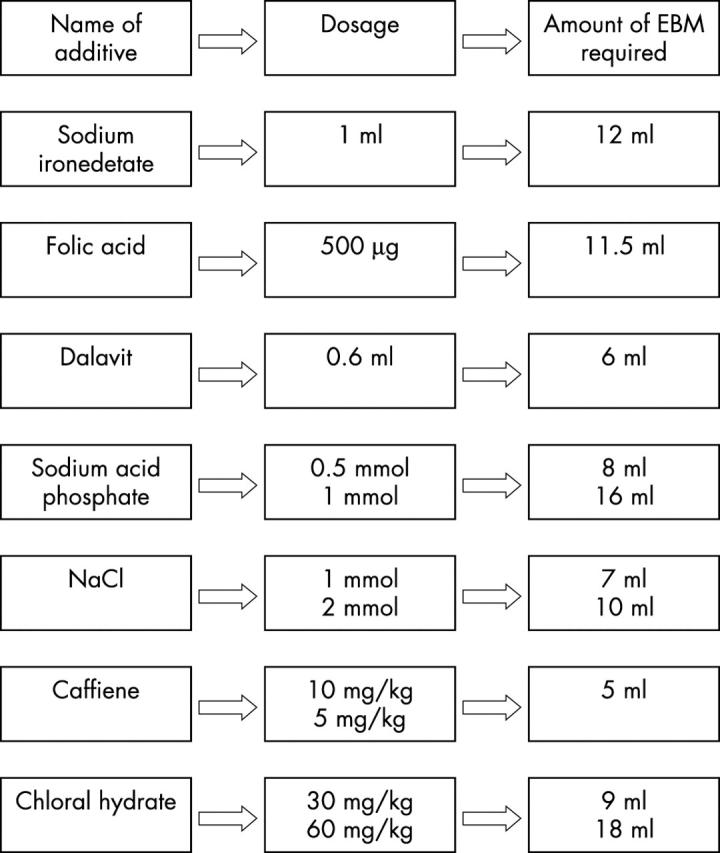
Amount of expressed breast milk required as solvent to maintain osmolality below 400 mOsm/kg.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Book L. S., Herbst J. J., Atherton S. O., Jung A. L. Necrotizing enterocolitis in low-birth-weight infants fed an elemental formula. J Pediatr. 1975 Oct;87(4):602–605. doi: 10.1016/s0022-3476(75)80835-3. [DOI] [PubMed] [Google Scholar]
- De Curtis M., Candusso M., Pieltain C., Rigo J. Effect of fortification on the osmolality of human milk. Arch Dis Child Fetal Neonatal Ed. 1999 Sep;81(2):F141–F143. doi: 10.1136/fn.81.2.f141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ernst J. A., Williams J. M., Glick M. R., Lemons J. A. Osmolality of substances used in the intensive care nursery. Pediatrics. 1983 Sep;72(3):347–352. [PubMed] [Google Scholar]
- Fenton Tanis R., Belik Jaques. Routine handling of milk fed to preterm infants can significantly increase osmolality. J Pediatr Gastroenterol Nutr. 2002 Sep;35(3):298–302. doi: 10.1097/00005176-200209000-00011. [DOI] [PubMed] [Google Scholar]
- Laker M. F., Menzies I. S. Increase in human intestinal permeability following ingestion of hypertonic solutions. J Physiol. 1977 Mar;265(3):881–894. doi: 10.1113/jphysiol.1977.sp011750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Le Guennec J. C., Paré C., Billon B. Hyperosmolar formulas in necrotizing enterocolitis. Am J Dis Child. 1983 May;137(5):506–506. doi: 10.1001/archpedi.1983.02140310084028. [DOI] [PubMed] [Google Scholar]
- Lucas A., Cole T. J. Breast milk and neonatal necrotising enterocolitis. Lancet. 1990 Dec 22;336(8730):1519–1523. doi: 10.1016/0140-6736(90)93304-8. [DOI] [PubMed] [Google Scholar]
- Lucas A., Morley R., Cole T. J., Lister G., Leeson-Payne C. Breast milk and subsequent intelligence quotient in children born preterm. Lancet. 1992 Feb 1;339(8788):261–264. doi: 10.1016/0140-6736(92)91329-7. [DOI] [PubMed] [Google Scholar]
- McGuire W., Anthony M. Y. Donor human milk versus formula for preventing necrotising enterocolitis in preterm infants: systematic review. Arch Dis Child Fetal Neonatal Ed. 2003 Jan;88(1):F11–F14. doi: 10.1136/fn.88.1.F11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schanler R. J., Shulman R. J., Lau C. Feeding strategies for premature infants: beneficial outcomes of feeding fortified human milk versus preterm formula. Pediatrics. 1999 Jun;103(6 Pt 1):1150–1157. doi: 10.1542/peds.103.6.1150. [DOI] [PubMed] [Google Scholar]
- Singhal A., Cole T. J., Lucas A. Early nutrition in preterm infants and later blood pressure: two cohorts after randomised trials. Lancet. 2001 Feb 10;357(9254):413–419. doi: 10.1016/S0140-6736(00)04004-6. [DOI] [PubMed] [Google Scholar]
- White K. C., Harkavy K. L. Hypertonic formula resulting from added oral medications. Am J Dis Child. 1982 Oct;136(10):931–933. doi: 10.1001/archpedi.1982.03970460061013. [DOI] [PubMed] [Google Scholar]
- Willis D. M., Chabot J., Radde I. C., Chance G. W. Unsuspected hyperosmolality of oral solutions contributing to necrotizing enterocolitis in very-low-birth-weight infants. Pediatrics. 1977 Oct;60(4):535–538. [PubMed] [Google Scholar]