

Abstract
AIMS—To develop appropriate methods of eye muscle surgery in highly myopic patients with esotropia and hypotropia, with respect to the pathological findings in high resolution magnetic resonance imaging (MRI). METHODS—35 patients with unilateral or bilateral high myopia and strabismus—that is, axial length of the globe averaged 29.4 mm. Multiple coronal, transverse, and parasagittal MRI image planes were obtained using a Siemens Magnetom 1.5 tesla MRI scanner. In 15 patients with a pathological plane of recti extraocular muscles found by MRI and confirmed intraoperatively, a new technique of eye muscle surgery was performed to re-establish the physiological muscle plane. This was checked postoperatively in addition to the measurement of alignment and motility by MRI. RESULTS—The new MRI finding of a dislocation of the lateral rectus (LR) into the temporocaudal quadrant by 3.4 mm requires new surgical techniques. Only fixing the LR in the physiological meridian at the equator with a silicone loop (`guide pulley') or a non-absorbable suture is a causal therapy. This yields alignment and improves abduction and elevation. CONCLUSIONS—If the described misalignment of the LR is detected by MRI, a common high dosage recess-resect procedure for esotropia may even aggravate the deviation. The most important aim of eye muscle surgery is to normalise the pathological path of the LR. The restoration of the physiological function of the dislocated LR is remarkable.
Full Text
The Full Text of this article is available as a PDF (235.1 KB).
Figure 1 .
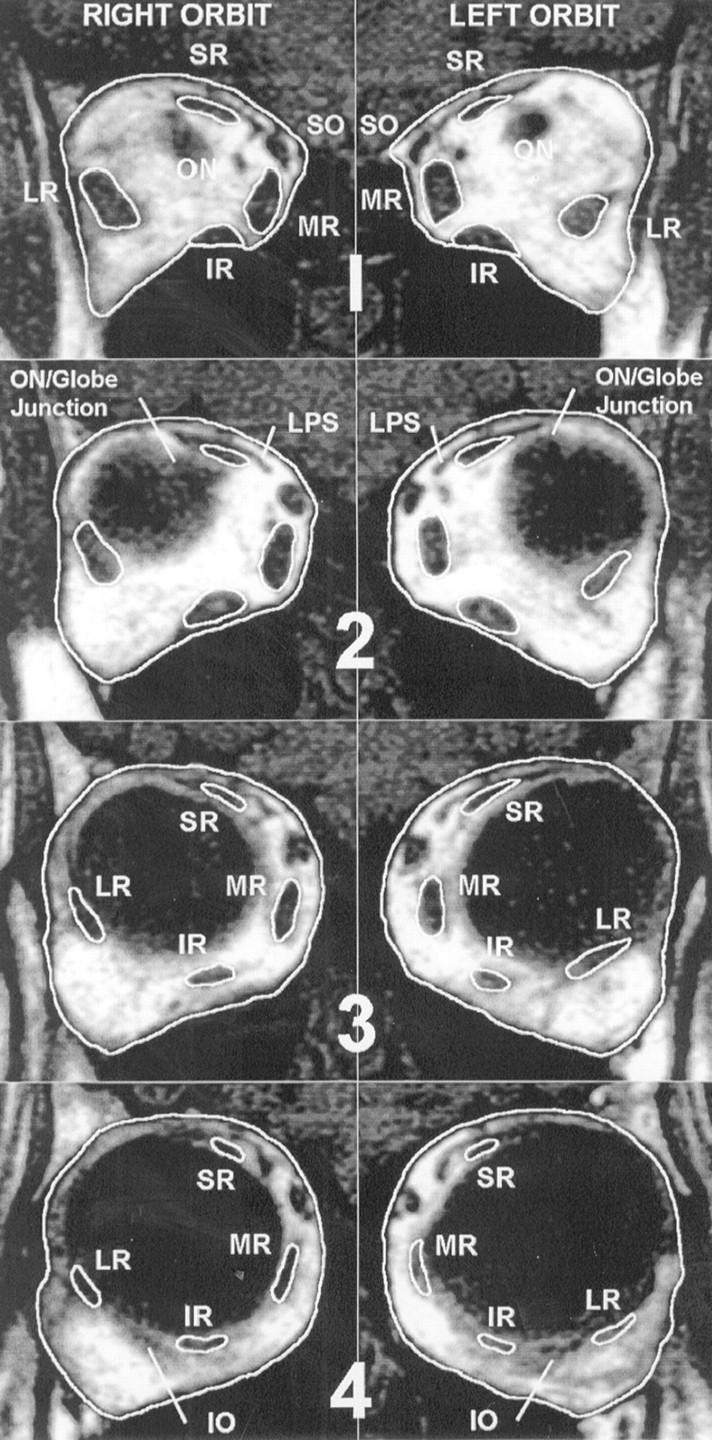
Coronal magnetic resonance image (T1 weighted, spin echo) of the right and left orbit of a characteristic subject (RG) in group 1 (Table 1). Images were obtained preoperatively fixing with the right eye in 10°downgaze and 5°adduction. From the images obtained at multiple levels of the orbit (from posterior, top (1) to anterior, bottom—that is, insertion site, (4, right)), the mislocation of the left lateral rectus (LR) into the lower temporal quadrant by 6 mm becomes obvious in the scans of the mid orbital region in (2). In this subject, even the insertion site of the left LR is shifted downwards as a result of previous surgery.
Figure 2 .
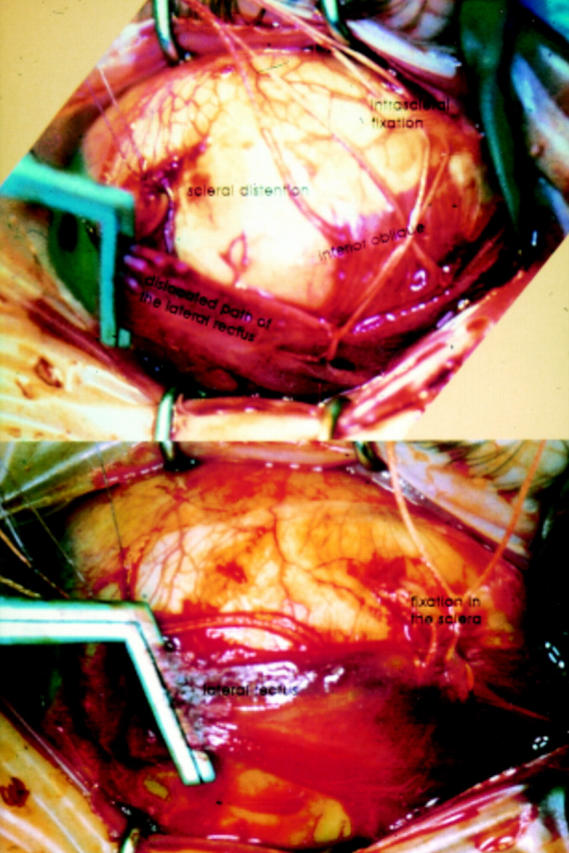
Top. Intraoperative situs of subject HJ in group 1 (Table 1). After recession of the MR by 16 mm, the LR is resected by 12 mm in the usual way and sutured with Vicryl 6/0 to the site of the original insertion. The path of the LR is still dislocated into the temporocaudal quadrant of the globe and orbit, caused by the scleral distension. Owing to this dislocation, the insertion site of the inferior oblique, white suture as label, is visible above (cranially) the LR. Another non-absorbable 4/0 suture is already in one third of the LR and fixed intrasclerally, the surgical knot not yet tightened. Bottom. The left LR is now fixed with a non-absorbable 4-0 suture (white Suturamid) in the sclera in the way of a modified retroequatorial myopexia in the physiological meridian.
Figure 3 .

Top (1-3). Parasagittal magnetic resonance image (MRI) scans of the left orbit of subject RG (Table 1) (group 1). The left MRI shows the normal plane of the inferior rectus in order to compare it with scan no 2, which shows the dislocated path of the LR. This obvious dislocation is not caused by the direction of gaze (downgaze). Scan no 3 (gaze ahead) demonstrates the postoperative surgically normalised path of left LR, which was fixed with a silicone loop and non-absorbable sutures in the sclera. Bottom (A-C). Coronal MRI of patient RG 2 weeks after eye muscle surgery of the left eye: the MR was recessed 10 mm and the LR was resected 8 mm and fixed more cranially. The silicone itself is visible as a black loop encircling the LR on the magnification below scan (C). Thus, the left LR is approximately 4 mm above the physiological horizontal meridian to prevent a renewed shifting in this case with high downward pulling force of the LR.
Figure 4 .

Deviations measured on the tangent screen at a distance of 2.5 metres in nine positions of gaze in a typical patient in group 1 with a dislocation of the right LR, simulated with the program ORBIT 1.5.1 (Miller and Shamaeva15). In each rectangle the upper left field indicates the value of the horizontal deviation (`+' for esotropia), the upper right the value of the vertical deviation (`+' for left eye hypotropia—that is, +VD) and the lower field shows the cyclotropia. Subject fixating with the left eye, in which the motility is not restricted. Note the V pattern esotropia of 16° versus 8° of esotropia. The more the eye is abducted, the more the LR becomes a depressor. This will result in increased esotropia and hypotropia in abduction.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Apt L. An anatomical reevaluation of rectus muscle insertions. Trans Am Ophthalmol Soc. 1980;78:365–375. [PMC free article] [PubMed] [Google Scholar]
- Bagolini B., Tamburrelli C., Dickmann A., Colosimo C. Convergent strabismus fixus in high myopic patients. Doc Ophthalmol. 1990 Apr-Jul;74(4):309–320. doi: 10.1007/BF00145815. [DOI] [PubMed] [Google Scholar]
- Demer J. L., Miller J. M., Poukens V., Vinters H. V., Glasgow B. J. Evidence for fibromuscular pulleys of the recti extraocular muscles. Invest Ophthalmol Vis Sci. 1995 May;36(6):1125–1136. [PubMed] [Google Scholar]
- Demer J. L., Von Noorden G. K. High myopia as an unusual cause of restrictive motility disturbance. Surv Ophthalmol. 1989 Jan-Feb;33(4):281–284. doi: 10.1016/0039-6257(82)90154-0. [DOI] [PubMed] [Google Scholar]
- Herzau V., Ioannakis K. Zur Pathogenese der Eso- und Hypotropie bei hoher Myopie. Klin Monbl Augenheilkd. 1996 Jan;208(1):33–36. doi: 10.1055/s-2008-1035165. [DOI] [PubMed] [Google Scholar]
- Hugonnier R., Magnard P. Les déséquilibres oculo-moteurs observés en cas de myopie forte. Ann Ocul (Paris) 1969 Jul;202(7):713–724. [PubMed] [Google Scholar]
- Taylor R., Whale K., Raines M. The heavy eye phenomenon: orthoptic and ophthalmic characteristics. Ger J Ophthalmol. 1995 Jul;4(4):252–255. [PubMed] [Google Scholar]