

Abstract
BACKGROUND/AIM—Patients with thyroid eye disease with upper eyelid retraction often develop overaction of the accessory muscles of eyelid closure, the glabellar muscles corrugator supercilii and procerus. The resultant glabellar furrowing (frown lines) contributes to the typical thyroid facies. The aim of this study was to evaluate the use of botulinum toxin A reversible chemodenervation of the glabellar muscles as adjunctive treatment in the rehabilitation of patients with thyroid eye disease. METHODS—14 patients (13 females) ages 39-76 years (mean 52) with inactive thyroid eye disease and associated medial eyebrow ptosis and prominent glabellar frown lines were recruited. All patients had a history of upper eyelid retraction. Each patient was treated with a single botulinum toxin injection (Dysport 0.2 ml, 40 units) into each corrugator supercilii and sometimes procerus muscles as an outpatient procedure. The effectiveness and acceptability of the treatment was assessed clinically and from a patient questionnaire. RESULTS—The injections were tolerated by 13/14 (93%) patients. There was resultant flattening of the glabellar region and improvement of medial eyebrow contour in all patients, with onset of paralysis within 1 week. All patients reported a subjective improvement in appearance. Side effects included one patient (7%) with reversible partial ptosis. The beneficial effect lasted 4-6 months, with a gradual return of function. Repeat treatment was indicated where there was persistent upper eyelid retraction and protractor overaction. CONCLUSION—Botulinum toxin A chemodenervation of the glabellar muscles in these patients was effective and acceptable. Chemodenervation should be considered in the rehabilitation of patients with thyroid eye disease where there is upper eyelid retraction and overacting protractors resulting in a thyroid frown. Once the eyelid retraction has been successfully treated by surgery, the need for further glabella muscle chemodenervation is considerably reduced. Keywords: botulinum toxin A; corrugator supercilii; frown lines; thyroid eye disease
Full Text
The Full Text of this article is available as a PDF (158.1 KB).
Figure 1 .

The corrugator supercilii muscles interdigitate with both frontalis and orbicularis at the medial end of the eyebrow.
Figure 2 .
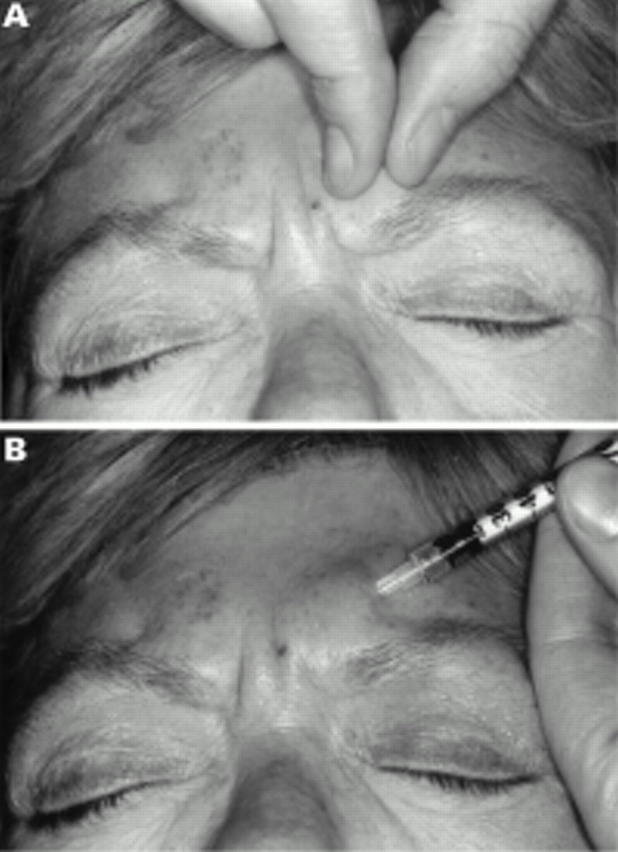
(A) Corrugator supercilii is easily palpated by asking the patient to contract these muscles. (B) Botulinum toxin A is injected diagonally through the thick glabellar skin into the bulk of the muscle. The needle is directed medial and inferiorly. The muscle must be relaxed during the injection to reduce discomfort.
Figure 3 .

This 67 year old female thyroid patient had bilateral upper eyelid retraction for 5 years. Two years after bilateral Henderson's procedures, she still had prominent glabellar lines and bunching of the medial end of the eyebrows. She received botulinum toxin A injections into both corrugator supercilii and procerus muscles. After treatment she could not contract her glabellar muscles even with the greatest effort—the glabellar region remained smooth while the palpebral apertures narrowed (orbicularis oculi) and lateral nasal folds formed (nasalis) from increased facial nerve activity. These photographs show the pretreatment, early post-treatment (2 weeks) and longer term post-treatment (4 months) effects. Glabellar region: (A) Pretreatment. Relaxed. (B) Pretreatment. Actively contracting. (C) Two weeks after treatment. Relaxed. (D) Two weeks after treatment. Actively trying to contract. (E) Four months after treatment. Relaxed. (F) Four months after treatment. Actively trying to contract.
Figure 4 .
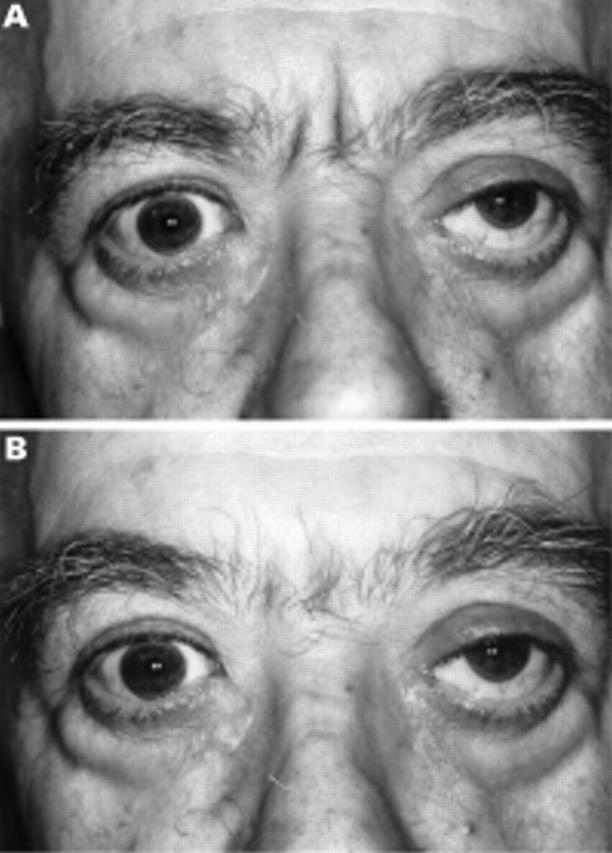
This 62 year old male thyroid patient had bilateral marked upper eyelid retraction for several years. Four months following bilateral levator recession he still had mild right upper eyelid retraction with marked glabellar furrows and altered eyebrow contour with bunched medial eyebrow ptosis. He received botulinum toxin A into the corrugator muscles but not procerus. After treatment the glabellar region was smoother but the established furrows were still visible. There was improvement of eyebrow contour by elevation and lateral displacement of the medial eyebrow. (A) Pretreatment. Relaxed. (B) One week after treatment. Relaxed.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Abramo A. C. Anatomy of the forehead muscles: the basis for the videoendoscopic approach in forehead rhytidoplasty. Plast Reconstr Surg. 1995 Jun;95(7):1170–1177. doi: 10.1097/00006534-199506000-00005. [DOI] [PubMed] [Google Scholar]
- Adams G. G., Kirkness C. M., Lee J. P. Botulinum toxin A induced protective ptosis. Eye (Lond) 1987;1(Pt 5):603–608. doi: 10.1038/eye.1987.93. [DOI] [PubMed] [Google Scholar]
- Borodic G. E., Cozzolino D. Blepharospasm and its treatment, with emphasis on the use of botulinum toxin. Plast Reconstr Surg. 1989 Mar;83(3):546–554. doi: 10.1097/00006534-198903000-00028. [DOI] [PubMed] [Google Scholar]
- Brin M. F., Fahn S., Moskowitz C., Friedman A., Shale H. M., Greene P. E., Blitzer A., List T., Lange D., Lovelace R. E. Localized injections of botulinum toxin for the treatment of focal dystonia and hemifacial spasm. Adv Neurol. 1988;50:599–608. [PubMed] [Google Scholar]
- Carruthers J. D., Carruthers J. A. Treatment of glabellar frown lines with C. botulinum-A exotoxin. J Dermatol Surg Oncol. 1992 Jan;18(1):17–21. doi: 10.1111/j.1524-4725.1992.tb03295.x. [DOI] [PubMed] [Google Scholar]
- Carruthers J., Stubbs H. A. Botulinum toxin for benign essential blepharospasm, hemifacial spasm and age-related lower eyelid entropion. Can J Neurol Sci. 1987 Feb;14(1):42–45. doi: 10.1017/s0317167100026159. [DOI] [PubMed] [Google Scholar]
- Clark R. P., Berris C. E. Botulinum toxin: a treatment for facial asymmetry caused by facial nerve paralysis. Plast Reconstr Surg. 1989 Aug;84(2):353–355. [PubMed] [Google Scholar]
- Clarke J. R., Spalton D. J. Treatment of senile entropion with botulinum toxin. Br J Ophthalmol. 1988 May;72(5):361–362. doi: 10.1136/bjo.72.5.361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dutton J. J. Botulinum-A toxin in the treatment of craniocervical muscle spasms: short- and long-term, local and systemic effects. Surv Ophthalmol. 1996 Jul-Aug;41(1):51–65. doi: 10.1016/s0039-6257(97)81995-9. [DOI] [PubMed] [Google Scholar]
- Elston J. S. Long-term results of treatment of idiopathic blepharospasm with botulinum toxin injections. Br J Ophthalmol. 1987 Sep;71(9):664–668. doi: 10.1136/bjo.71.9.664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fitzsimons R., Lee J. P., Elston J. Treatment of sixth nerve palsy in adults with combined botulinum toxin chemodenervation and surgery. Ophthalmology. 1988 Nov;95(11):1535–1542. doi: 10.1016/s0161-6420(88)32976-3. [DOI] [PubMed] [Google Scholar]
- Foster J. A., Barnhorst D., Papay F., Oh P. M., Wulc A. E. The use of botulinum A toxin to ameliorate facial kinetic frown lines. Ophthalmology. 1996 Apr;103(4):618–622. doi: 10.1016/s0161-6420(96)30644-1. [DOI] [PubMed] [Google Scholar]
- Frueh B. R., Felt D. P., Wojno T. H., Musch D. C. Treatment of blepharospasm with botulinum toxin. A preliminary report. Arch Ophthalmol. 1984 Oct;102(10):1464–1468. doi: 10.1001/archopht.1984.01040031184014. [DOI] [PubMed] [Google Scholar]
- Frueh B. R., Musch D. C. Treatment of facial spasm with botulinum toxin. An interim report. Ophthalmology. 1986 Jul;93(7):917–923. doi: 10.1016/s0161-6420(86)33641-8. [DOI] [PubMed] [Google Scholar]
- Gonnering R. S. Treatment of hemifacial spasm with botulinum A toxin. Results and rationale. Ophthal Plast Reconstr Surg. 1986;2(3):143–146. doi: 10.1097/00002341-198601060-00005. [DOI] [PubMed] [Google Scholar]
- Grandas F., Elston J., Quinn N., Marsden C. D. Blepharospasm: a review of 264 patients. J Neurol Neurosurg Psychiatry. 1988 Jun;51(6):767–772. doi: 10.1136/jnnp.51.6.767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guyuron B., Huddleston S. W. Aesthetic indications for botulinum toxin injection. Plast Reconstr Surg. 1994 Apr;93(5):913–918. doi: 10.1097/00006534-199404001-00003. [DOI] [PubMed] [Google Scholar]
- Keen M., Blitzer A., Aviv J., Binder W., Prystowsky J., Smith H., Brin M. Botulinum toxin A for hyperkinetic facial lines: results of a double-blind, placebo-controlled study. Plast Reconstr Surg. 1994 Jul;94(1):94–99. doi: 10.1097/00006534-199407000-00009. [DOI] [PubMed] [Google Scholar]
- Lemke B. N., Stasior O. G. The anatomy of eyebrow ptosis. Arch Ophthalmol. 1982 Jun;100(6):981–986. doi: 10.1001/archopht.1982.01030030989019. [DOI] [PubMed] [Google Scholar]
- Letourneau A., Daniel R. K. The superficial musculoaponeurotic system of the nose. Plast Reconstr Surg. 1988 Jul;82(1):48–57. [PubMed] [Google Scholar]
- Lingua R. W. Sequelae of botulinum toxin injection. Am J Ophthalmol. 1985 Aug 15;100(2):305–307. doi: 10.1016/0002-9394(85)90797-4. [DOI] [PubMed] [Google Scholar]
- Patrinely J. R., Whiting A. S., Anderson R. L. Local side effects of botulinum toxin injections. Adv Neurol. 1988;49:493–500. [PubMed] [Google Scholar]
- Piérard G. E., Lapière C. M. The microanatomical basis of facial frown lines. Arch Dermatol. 1989 Aug;125(8):1090–1092. doi: 10.1001/archderm.1989.01670200066010. [DOI] [PubMed] [Google Scholar]
- Ramirez O. M. The anchor subperiosteal forehead lift. Plast Reconstr Surg. 1995 May;95(6):993–1006. [PubMed] [Google Scholar]
- Scott A. B. Botulinum toxin injection of eye muscles to correct strabismus. Trans Am Ophthalmol Soc. 1981;79:734–770. [PMC free article] [PubMed] [Google Scholar]
- Scott A. B., Kennedy R. A., Stubbs H. A. Botulinum A toxin injection as a treatment for blepharospasm. Arch Ophthalmol. 1985 Mar;103(3):347–350. doi: 10.1001/archopht.1985.01050030043017. [DOI] [PubMed] [Google Scholar]
- Shorr N., Seiff S. R., Kopelman J. The use of botulinum toxin in blepharospasm. Am J Ophthalmol. 1985 May 15;99(5):542–546. doi: 10.1016/s0002-9394(14)77954-1. [DOI] [PubMed] [Google Scholar]
- Taylor J. D., Kraft S. P., Kazdan M. S., Flanders M., Cadera W., Orton R. B. Treatment of blepharospasm and hemifacial spasm with botulinum A toxin: a Canadian multicentre study. Can J Ophthalmol. 1991 Apr;26(3):133–138. [PubMed] [Google Scholar]