

Abstract
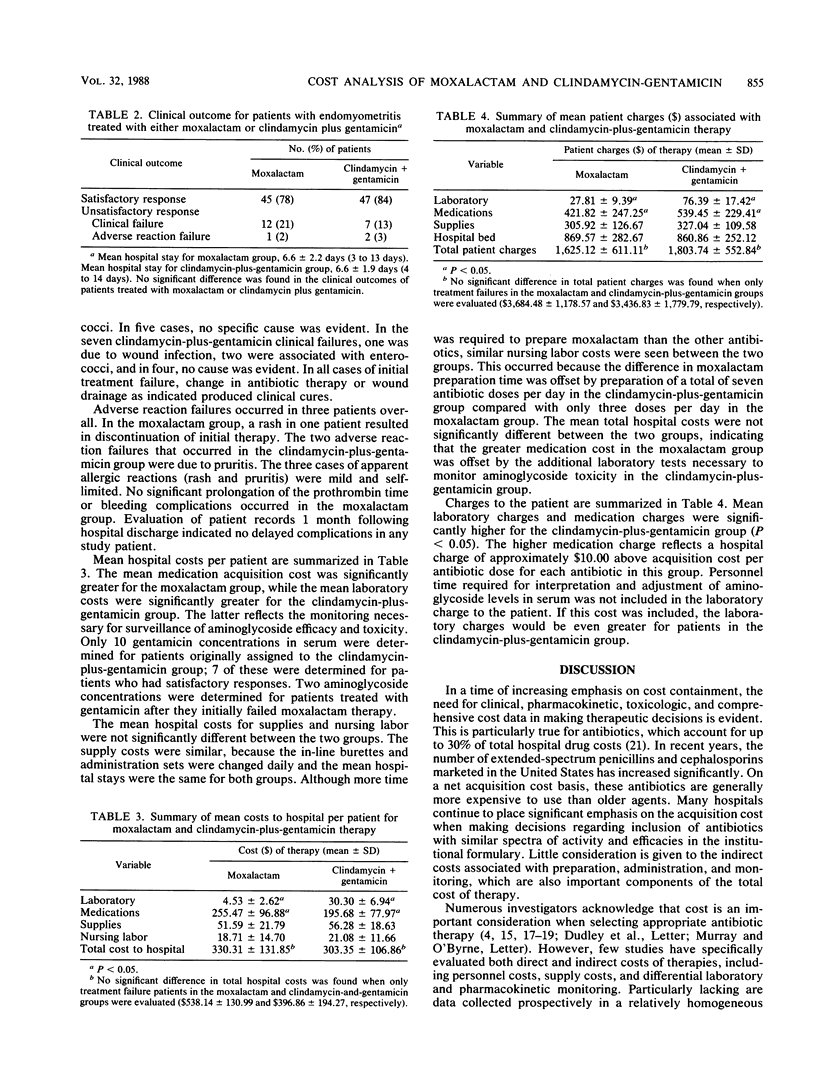
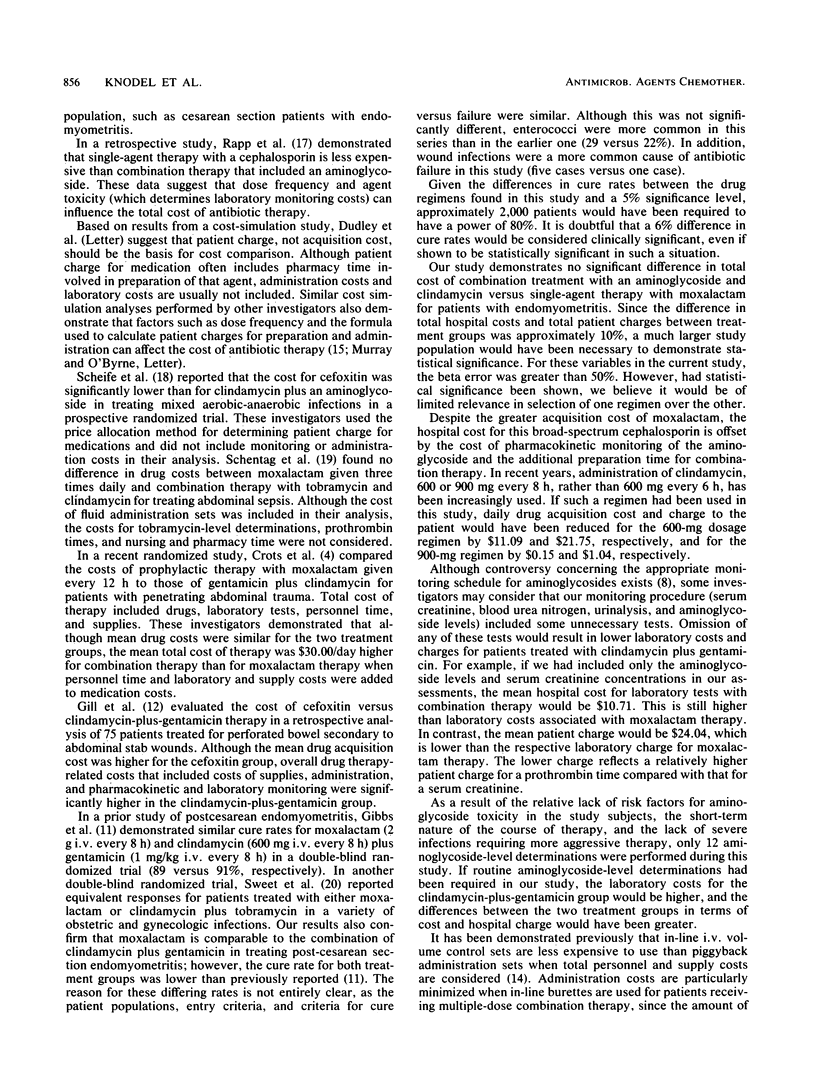
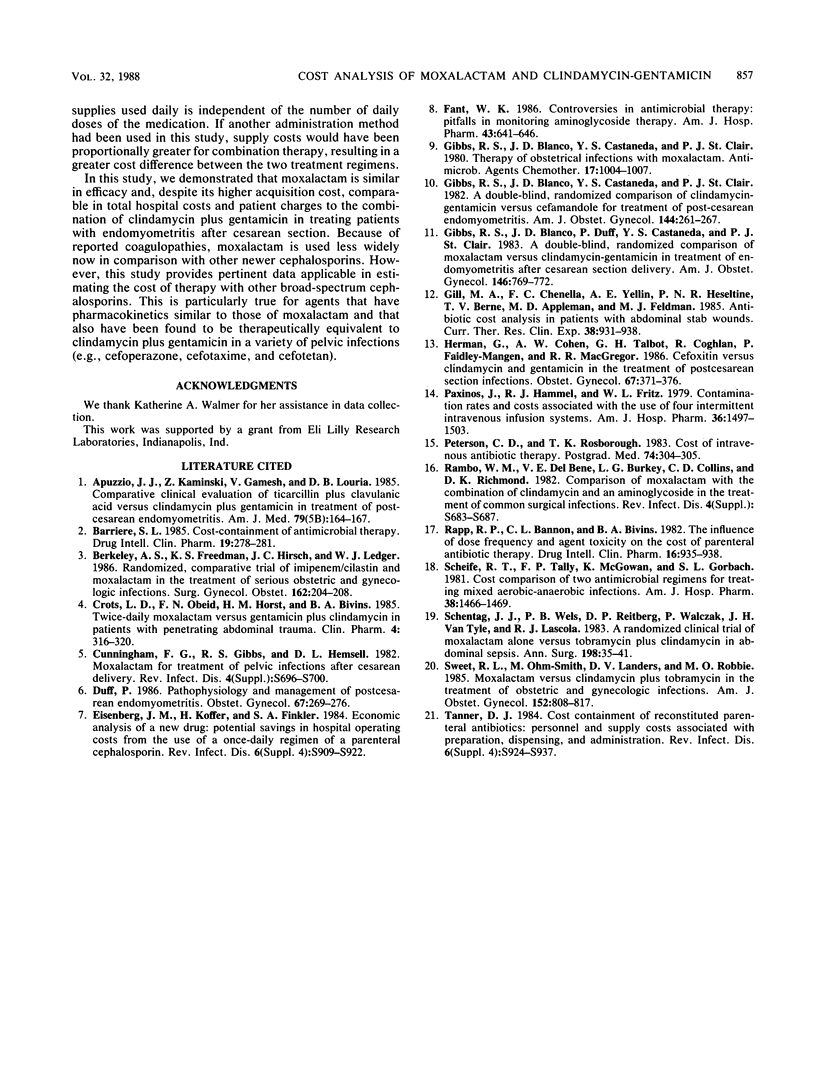
The direct and indirect costs associated with either moxalactam or clindamycin plus gentamicin as treatment for endomyometritis after emergent cesarean section were compared in an open, randomized prospective trial of 114 patients. A total of 58 patients were assigned to receive moxalactam, 2 g intravenously (i.v.) every 8 h for 5 doses, followed by 2 g every 12 h and prophylactic vitamin K (10 mg) intramuscularly, and 56 patients were assigned to receive clindamycin (600 mg) i.v. every 6 h plus gentamicin (1.5 mg/kg) i.v. every 8 h. Prothrombin times were measured in moxalactam-treated patients, and patients treated with clindamycin plus gentamicin had urinalyses and blood urea nitrogen and serum creatinine determinations performed before and after treatment. Also, gentamicin levels in serum were determined as clinically indicated. A satisfactory treatment response was defined as the resolution of signs and symptoms of endomyometritis within 3 days of the start of antibiotic therapy. Satisfactory responses were demonstrated in 78% of the moxalactam-treated patients and 84% of patients treated with clindamycin plus gentamicin. Mean hospital costs for laboratory tests ($30.30 versus $4.53) and mean patient charges for laboratory tests ($76.39 versus $27.81) and medications ($539.45 versus $421.82) were significantly higher in patients treated with clindamycin plus gentamicin (P less than 0.05), while mean medication costs to the hospital were greater in the moxalactam group ($255.47 versus $195.68; P less than 0.05). However, total patient charges and total hospital drug-associated costs were not significantly different for the two group. In this tudy, moxalactam was similar in efficacy and, despite its higher acquistion cost, was comparable in total hospital costs and patient charges to clindamycin plus gentacmicin in treating endomyometritis.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Apuzzio J. J., Kaminski Z., Gamesh V., Louria D. B. Comparative clinical evaluation of ticarcillin plus clavulanic acid versus clindamycin plus gentamicin in treatment of post-cesarean endomyometritis. Am J Med. 1985 Nov 29;79(5B):164–167. doi: 10.1016/0002-9343(85)90152-4. [DOI] [PubMed] [Google Scholar]
- Barriere S. L. Cost-containment of antimicrobial therapy. Drug Intell Clin Pharm. 1985 Apr;19(4):278–281. doi: 10.1177/106002808501900405. [DOI] [PubMed] [Google Scholar]
- Berkeley A. S., Freedman K. S., Hirsch J. C., Ledger W. J. Randomized, comparative trial of imipenem/cilastatin and moxalactam in the treatment of serious obstetric and gynecologic infections. Surg Gynecol Obstet. 1986 Mar;162(3):204–208. [PubMed] [Google Scholar]
- Crots L. D., Obeid F. N., Horst H. M., Bivins B. A. Twice-daily moxalactam versus gentamicin and clindamycin in patients with penetrating abdominal trauma. Clin Pharm. 1985 May-Jun;4(3):316–320. [PubMed] [Google Scholar]
- Cunningham F. G., Gibbs R. S., Hemsell D. L. Moxalactam for treatment of pelvic infections after cesarean delivery. Rev Infect Dis. 1982 Nov-Dec;4 (Suppl):S696–S700. doi: 10.1093/clinids/4.supplement_3.s696. [DOI] [PubMed] [Google Scholar]
- Duff P. Pathophysiology and management of postcesarean endomyometritis. Obstet Gynecol. 1986 Feb;67(2):269–276. doi: 10.1097/00006250-198602000-00021. [DOI] [PubMed] [Google Scholar]
- Eisenberg J. M., Koffer H., Finkler S. A. Economic analysis of a new drug: potential savings in hospital operating costs from the use of a once-daily regimen of a parenteral cephalosporin. Rev Infect Dis. 1984 Nov-Dec;6 (Suppl 4):S909–S923. doi: 10.1093/clinids/6.supplement_4.s909. [DOI] [PubMed] [Google Scholar]
- Fant W. K. Controversies in antimicrobial therapy: pitfalls in monitoring aminoglycoside therapy. Am J Hosp Pharm. 1986 Mar;43(3):641–646. [PubMed] [Google Scholar]
- Gibbs R. S., Blanco J. D., Castaneda Y. S., St Clair P. J. A double-blind, randomized comparison of clindamycin-gentamicin versus cefamandole for treatment of post-cesarean section endomyometritis. Am J Obstet Gynecol. 1982 Oct 1;144(3):261–267. doi: 10.1016/0002-9378(82)90576-2. [DOI] [PubMed] [Google Scholar]
- Gibbs R. S., Blanco J. D., Castaneda Y. S., St Clair P. J. Therapy of obstetrical infections with moxalactam. Antimicrob Agents Chemother. 1980 Jun;17(6):1004–1007. doi: 10.1128/aac.17.6.1004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibbs R. S., Blanco J. D., Duff P., Castaneda Y. S., St Clair P. J. A double-blind, randomized comparison of moxalactam versus clindamycin-gentamicin in treatment of endomyometritis after cesarean section delivery. Am J Obstet Gynecol. 1983 Aug 1;146(7):769–772. doi: 10.1016/0002-9378(83)91075-x. [DOI] [PubMed] [Google Scholar]
- Herman G., Cohen A. W., Talbot G. H., Coghlan R., Faidley-Mangen P., MacGregor R. R. Cefoxitin versus clindamycin and gentamicin in the treatment of postcesarean section infections. Obstet Gynecol. 1986 Mar;67(3):371–376. [PubMed] [Google Scholar]
- Paxinos J., Hammel R. J., Fritz W. L. Contamination rates and costs associated with the use of four intermittent intravenous infusion systems. Am J Hosp Pharm. 1979 Nov;36(11):1497–1503. [PubMed] [Google Scholar]
- Peterson C. D., Rosborough T. K. Cost of intravenous antibiotic therapy. Frequency of administration as a factor. Postgrad Med. 1983 Sep;74(3):304–305. doi: 10.1080/00325481.1983.11698436. [DOI] [PubMed] [Google Scholar]
- Rambo W. M., Del Bene V. E., Burkey L. G., Collins C. D., Richmond D. K. Comparison of moxalactam with the combination of clindamycin and an aminoglycoside in the treatment of common surgical infections. Rev Infect Dis. 1982 Nov-Dec;4 (Suppl):S683–S687. [PubMed] [Google Scholar]
- Rapp R. P., Bannon C. L., Bivins B. A. The influence of dose frequency and agent toxicity on the cost of parenteral antibiotic therapy. Drug Intell Clin Pharm. 1982 Dec;16(12):935–938. doi: 10.1177/106002808201601207. [DOI] [PubMed] [Google Scholar]
- Scheife R. T., Tally F. P., McGowan K., Gorbach S. L. Cost comparison of two antimicrobial regimens for treating mixed aerobic-anaerobic infections. Am J Hosp Pharm. 1981 Oct;38(10):1466–1469. [PubMed] [Google Scholar]
- Schentag J. J., Wels P. B., Reitberg D. P., Walczak P., Van Tyle J. H., Lascola R. J. A randomized clinical trial of moxalactam alone versus tobramycin plus clindamycin in abdominal sepsis. Ann Surg. 1983 Jul;198(1):35–41. doi: 10.1097/00000658-198307000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sweet R. L., Ohm-Smith M., Landers D. V., Robbie M. O. Moxalactam versus clindamycin plus tobramycin in the treatment of obstetric and gynecologic infections. Am J Obstet Gynecol. 1985 Aug 1;152(7 Pt 1):808–817. doi: 10.1016/s0002-9378(85)80068-5. [DOI] [PubMed] [Google Scholar]
- Tanner D. J. Cost containment of reconstituted parenteral antibiotics: personnel and supply costs associated with preparation, dispensing, and administration. Rev Infect Dis. 1984 Nov-Dec;6 (Suppl 4):S924–S937. doi: 10.1093/clinids/6.supplement_4.s924. [DOI] [PubMed] [Google Scholar]