

Abstract
BACKGROUND—Standard examination of contrast sensitivity under conditions of glare disability is performed with incandescent light. A new halogen glare test that simulates glare as seen with oncoming vehicle headlights was used to measure glare disability in patients implanted with multifocal and monofocal intraocular lenses (IOLs). METHODS—28 patients with an average age of 69 years (SD 12 years) were implanted with a monofocal IOL (SI-40NB, Allergan) and 28 patients with an average of 66 years (12 years) were implanted with a refractive multifocal IOL (Array-SA-40N, Allergan). All patients were followed for 5 months postoperatively. Contrast sensitivity at four spatial frequencies (3, 6, 12, and 18 cycles per degree, cpd) with and without a glare source were measured using the halogen glare test (CSV-1000 HGT). Statistical analysis was performed using the two sample Wilcoxon test. The local significance level was set at 0.05. RESULTS—When tested at the lowest spatial frequency (3 cpd) without halogen glare, contrast sensitivity was lower in the multifocal group than in the monofocal group (p=0.0292). With additional glare, there was no difference between both groups. At all other spatial frequencies (6, 12, and 18 cpd), when tested without halogen glare (6 cpd, p=0.5250; 12 cpd, p=0.8483; 18 cpd, p=0.9496) and with moderate (3 cpd, p=0.7993; 6 cpd, p=0.4639; 12 cpd, p=0.7456; 18 cpd, p=1.0) and high halogen glare (3 cpd, p=0.1513; 6 cpd, p=0.2016; 12 cpd, p=0.3069; 18 cpd, p=0.9933), there was no statistically significant difference between groups. Patients in both groups of age 70 or older had reduced contrast sensitivity without halogen glare and with moderate and strong glare. When monofocal and multifocal patients older than 70 years of age were analysed separately, there was no statistically significant difference in contrast sensitivity with and without glare. Astigmatism >1 dioptre had no significant influence on contrast sensitivity and glare disability when monofocal and multifocal eyes were compared. CONCLUSION—Reduced contrast sensitivity was found in the multifocal group only at the lowest spatial frequency without halogen glare. The monofocal and multifocal groups had no statistically significant differences in contrast sensitivity with moderate and strong glare. These results suggest no difference in glare disability induced by halogen light similar to oncoming vehicle headlights for patients implanted with monofocal and multifocal IOLs.
Full Text
The Full Text of this article is available as a PDF (141.0 KB).
Figure 1 .

Halogen intraocular lenses glare test CSV-1000HGT at medium glare.
Figure 2 .
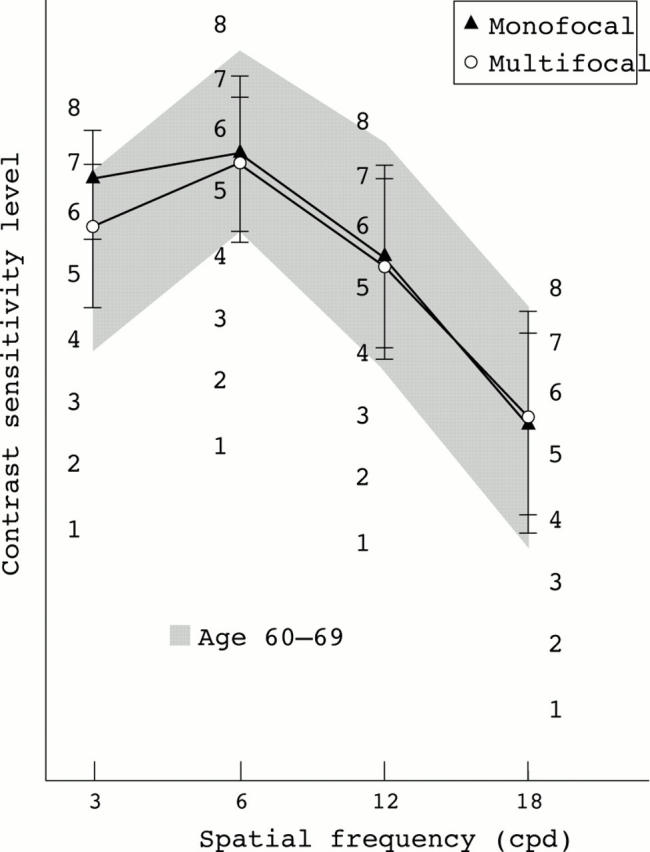
No glare: contrast sensitivity was statistically significantly lower for the multifocal group compared with the monofocal group only at the lowest spatial frequency of 3 cycles per degree (cpd).
Figure 3 .
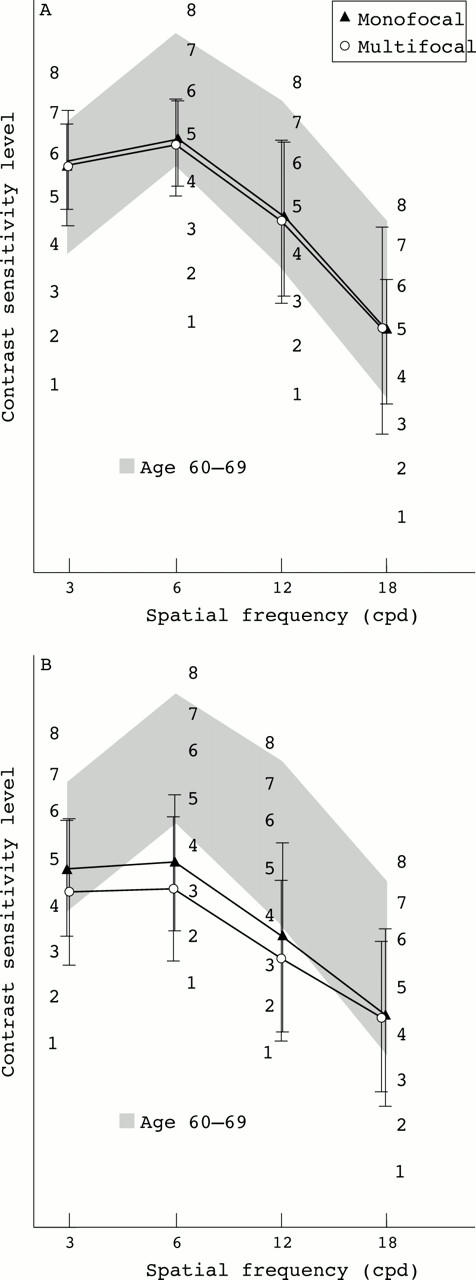
Moderate (A) and high glare (B). No statistically significant difference between both groups at any spatial frequency.
Figure 4 .
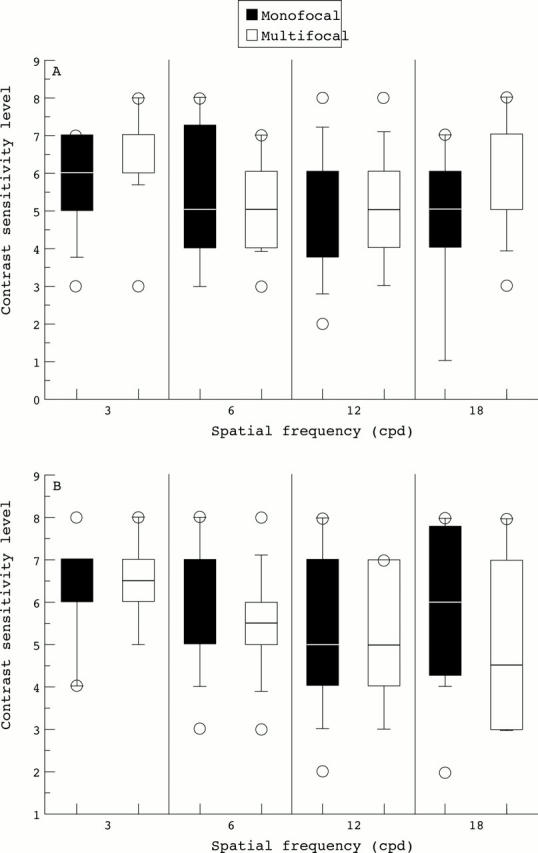
Separate analysis of monofocal versus and multifocal patients younger than 70 years (A) and older than 70 years (B): no statistically significant difference between both groups within the age groups at any spatial frequency.
Figure 5 .
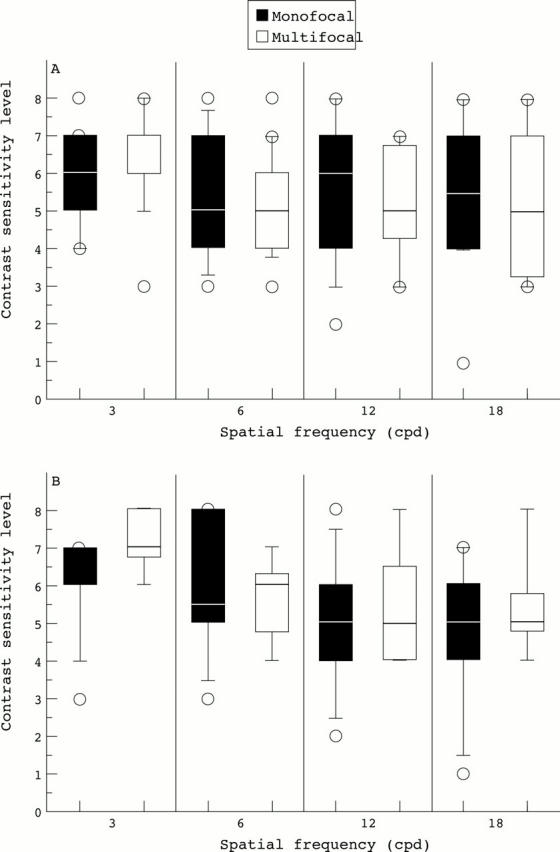
Astigmatism less than 1 dioptre (A) and more than 1 dioptre (B). Greater astigmatism had no statistically significant influence on contrast sensitivity or glare disability when monofocal eyes were compared with multifocal eyes.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Dick H. B., Krummenauer F., Schwenn O., Krist R., Pfeiffer N. Objective and subjective evaluation of photic phenomena after monofocal and multifocal intraocular lens implantation. Ophthalmology. 1999 Oct;106(10):1878–1886. doi: 10.1016/S0161-6420(99)90396-2. [DOI] [PubMed] [Google Scholar]
- Eisenmann D., Hessemer V., Manzke B., Stork W., Jacobi K. W. Modulationsübertragungsfunktion und Kontrastempfindlichkeit refraktiver Mehrzonenmultifokallinsen. Ophthalmologe. 1993 Aug;90(4):343–347. [PubMed] [Google Scholar]
- Eisenmann D., Jacobi F. K., Dick B., Jacobi K. W., Pabst W. Untersuchungen zur Blendempfindlichkeit phaker und pseudophaker Augen. Klin Monbl Augenheilkd. 1996 Feb;208(2):87–92. doi: 10.1055/s-2008-1035175. [DOI] [PubMed] [Google Scholar]
- Eisenmann D., Jacobi K. W. Die ARRAY-Multifokallinse--Funktionsprinzip und klinische Ergebnisse. Klin Monbl Augenheilkd. 1993 Sep;203(3):189–194. doi: 10.1055/s-2008-1045666. [DOI] [PubMed] [Google Scholar]
- Eisenmann D., Wagner R., Dick B., Jacobi K. W. Einfluss des Hornhautastigmatismus auf die Kontrastempfindlichkeit bei mono- und multifokaler Pseudophakie--eine theoretische Studie am physikalischen Auge. Klin Monbl Augenheilkd. 1996 Aug-Sep;209(2-3):125–131. doi: 10.1055/s-2008-1035291. [DOI] [PubMed] [Google Scholar]
- Holladay J. T., Van Dijk H., Lang A., Portney V., Willis T. R., Sun R., Oksman H. C. Optical performance of multifocal intraocular lenses. J Cataract Refract Surg. 1990 Jul;16(4):413–422. doi: 10.1016/s0886-3350(13)80793-6. [DOI] [PubMed] [Google Scholar]
- Jacobi P. C., Konen W. Effect of age and astigmatism on the AMO Array multifocal intraocular lens. J Cataract Refract Surg. 1995 Sep;21(5):556–561. doi: 10.1016/s0886-3350(13)80217-9. [DOI] [PubMed] [Google Scholar]
- Pomerance G. N., Evans D. W. Test-retest reliability of the CSV-1000 contrast test and its relationship to glaucoma therapy. Invest Ophthalmol Vis Sci. 1994 Aug;35(9):3357–3361. [PubMed] [Google Scholar]
- Rüther K., Eisenmann D., Zrenner E., Jacobi K. W. Der Einfluss diffraktiver Multifokallinsen auf Kontrastsehen, Gegenlichtsehschärfe und Farbsinn. Klin Monbl Augenheilkd. 1994 Jan;204(1):14–19. doi: 10.1055/s-2008-1035495. [DOI] [PubMed] [Google Scholar]
- Weatherill J., Yap M. Contrast sensitivity in pseudophakia and aphakia. Ophthalmic Physiol Opt. 1986;6(3):297–301. [PubMed] [Google Scholar]
- Westheimer G. Scaling of visual acuity measurements. Arch Ophthalmol. 1979 Feb;97(2):327–330. doi: 10.1001/archopht.1979.01020010173020. [DOI] [PubMed] [Google Scholar]