

Abstract
Amblyopia (“lazy eye”) is an impairment in visual acuity resulting from abnormal neural development in the visual cortex. We tested the responses of ten amblyopic and six normal observers to illusions of perceived orientation in textures of Gabor patches: the “Fraser illusion,” the “phase illusion,” and a “tilted chain” illusion. The illusory tilt of the stimulus rows was matched by actual tilt in the opposite direction by using the method of constant stimuli. Amblyopes showed a significant increase in the Fraser illusion, a decrease in the phase illusion, and a reversal of the tilted chain illusion. Amblyopic performance could be simulated in normal observers by reducing the length of the rows. These results can be modeled by a theory which places the neural abnormality in amblyopia at the level of second stage grouping processes. Additionally, the illusions might be useful in the early diagnosis of amblyopia without the need for prior refractive correction.
Amblyopia is a developmental visual impairment which cannot be eliminated by optical refraction (glasses), and has no clear organic cause, such as glaucoma, damage to the optic nerve, or damage to the retina (1). Amblyopia can be induced in animals by visual deprivation during critical periods of development, and is in these cases associated with specific neurophysiological and psychophysical abnormalities in the representation of visual space in the primary visual cortex (2). Amblyopia in humans is thought to be characterized by spatial undersampling (3–5), topographical jitter (3, 4, 6), impaired processing of spatial phase (7, 8), and contrast sensitivity loss (3). Illusions have proven to be very useful in understanding the neural mechanisms of normal pattern vision (9, 10), and here we show that illusions, or their absence, may also be diagnostic for amblyopic vision.
When visual information is processed veridically, there are many different algorithms or heuristics the visual system might use to achieve this. However, errors in visual processing can be informative about which particular heuristics (rules of thumb) and algorithms (structural rules) might actually operate in the visual cortex. Errors in visual processing occur in visual illusions. Careful comparisons among visual illusions can provide specific information about which heuristics are used by the visual system, and under what conditions. Errors in visual processing can also occur in neuropsychological patients, where some part of the visual cortex is damaged. Selective deficits of visual processing tell us about the functional organization of the cortical visual system (11). Although amblyopia is the result of developmental rather than accidental damage to the visual cortex, it is nonetheless of cortical etiology. Selective deficits in the appearance of visual illusions in amblyopia can inform us both about the nature of the associated visual impairment, and about normal visual processing.
In the Fraser illusion, a straight line composed of tilted elements itself appears tilted (12). Two-dimensional Gabor patches (sinusoidal grating modulated by a Gaussian envelope) can be detected at low contrasts, and their spatial layout resembles the receptive fields of simple visual neurons in V1 (13). Additionally, Gabor patches have well defined properties in both spatial and frequency domains. The Fraser illusion can be replicated by using a texture of elongated Gabor patches containing a tilted carrier grating (14) (Fig. 1a), or a texture of circular Gabor-patch elements successively shifted in phase (Fig. 1b; ref. 15). We discovered a tilted chain variant of this illusion, whereby a row of slightly tilted circular Gabor patches arranged in opposite contrast phase appears to tilt, surprisingly, not in the direction of the tilted elements but in the opposite direction (Fig. 1c). It is well known that at 10–15° the Fraser illusion melds over to the opposite Zöllner illusion (16), and indeed the fact that the energy of the tilted chain stimulus peaks in this orientation interval might contribute to the counterintuitive direction of the illusion. We have developed a model based on neural population coding of the orientations of both the internal black and white bars of the stimulus, and the axis of the stimulus as a whole (see Discussion).
Figure 1.
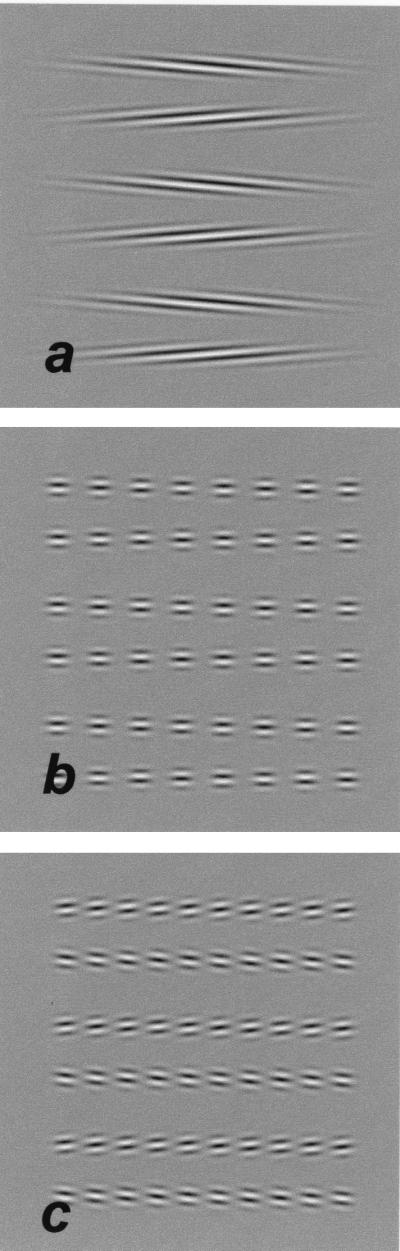
Tilt illusions. (a) Fraser illusion: the carrier is tilted by 5° to the envelope orientation. (b) Phase illusion: successive patches are shifted in phase by ¼ cycle. (c) Tilted-chain illusion: patches are tilted by 6° to the row orientation, such that successive patches are shifted by ½ cycle along the carrier. Two new orientations emerge.
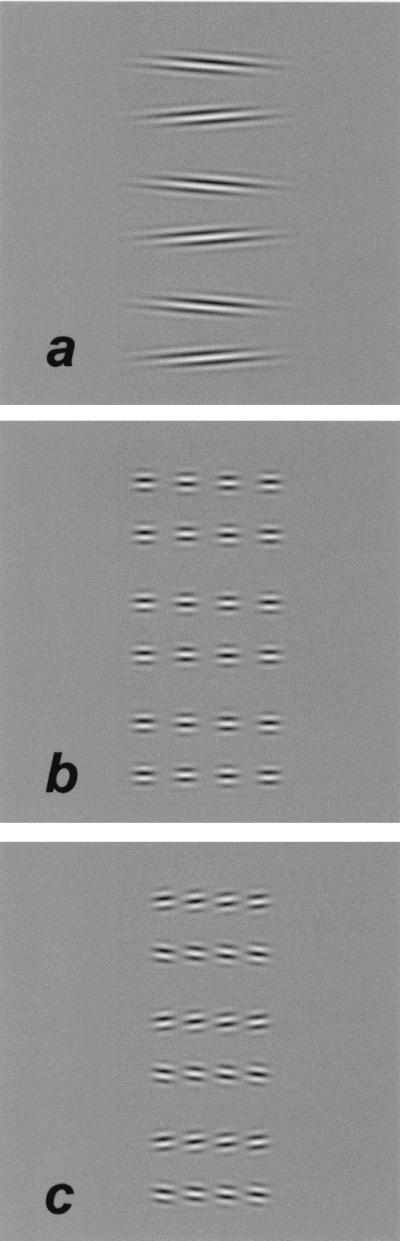
In general, illusions are enhanced by poor visibility, because the weak visual signal is more susceptible to bias (9). However, a tilt illusion composed of a texture of Gabor patches successively shifted in phase contains little redundancy of visual information. Fig. 2 shows the tilt illusions with the type of spatial degradations often associated with amblyopia (i.e., undersampling and positional uncertainty), and it is clear that whereas the Fraser illusion is preserved, the phase illusion is considerably reduced and the tilted chain illusion changes direction.
Figure 2.

The stimulus as it might be processed by amblyopes, with added noise to mimic the effects of amblyopia (sparse sampling, topographical jitter, and phase jitter). (a) Fraser illusion. (b) Phase illusion. (c) Tilted-chain illusion.
To learn how amblyopia affects the functional organization of the visual cortex, we measured the amount of tilt perceived in the illusion images (Fig. 1) in a group of amblyopes.
Method
Ten amblyopes and six normal observers (including the authors) participated in these experiments. All amblyopes had an interocular difference of at least two lines in an acuity chart. Where necessary, refractive correction was used. Six amblyopes were strabismic (having some degree of misalignment between the two eyes), of whom four also had more than two diopters of anisometropia. Four amblyopes were pure anisometropes, with different refractive errors in the two eyes, but no misalignment of the visual axes.
Stimuli (Figs. 1, 3, and 4) were 110-msec textures of Gabor patches (3 cycles per degree of visual angle sinusoidal grating in a two-dimensional Gaussian envelope of σ = 13.6 arcmin by 13.6 arcmin, or in the Fraser illusion x ⋅ 13.6 arcmin where 2 ≤ x ≤ 10), generated by CRS/VSG/3 graphics-cards in 586 Komputer PCs, presented on Mitsubishi Diamond-pro21TX (1024 × 1024 270-μm pixels) and Diamond-Scan20H (960 × 960 250 μm pixels), at 72 Hz, viewed from 120 cm and 110 cm, respectively, such that each pixel subtended about 0.75 arcmin of visual angle.
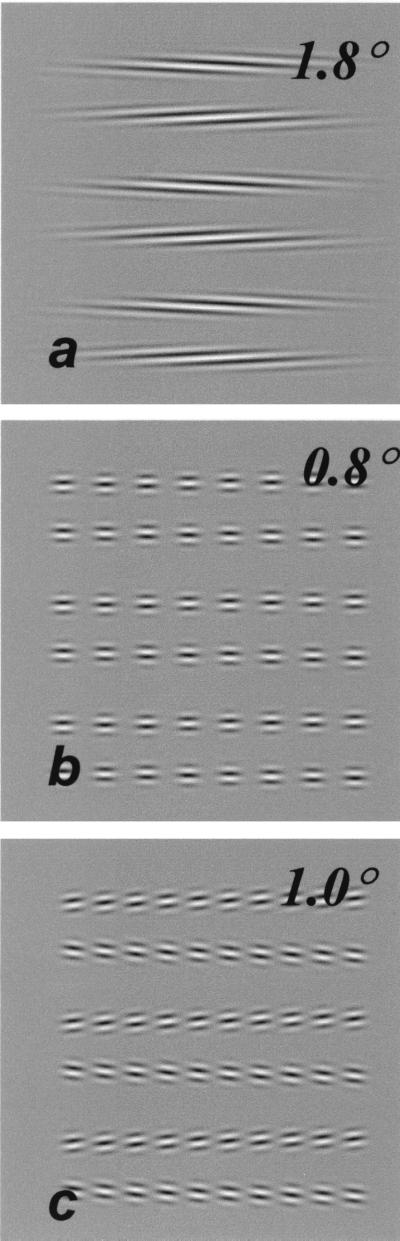
Figure 3.
The stimulus as it might be processed by amblyopes, with shorter rows. Normal responses to these shorter stimuli were similar to the amblyopes' responses to the stimuli in Fig. 1. (a) Fraser illusion. (b) Phase illusion. (c) Tilted chain illusion.
Figure 4.
Method: illusory tilt compensated by actual tilt in the opposite direction by the amount indicated. (a) Fraser illusion. (b) Phase illusion. (c) Tilted-chain illusion.
In experiment 1, we measured how much illusory tilt was perceived by a group of amblyopic observers who had impaired visual acuity in one eye, and a group of normal control observers. To control for poor visibility, some normal controls repeated this experiment with optical blurring. Blurring is a useful model only for pure anisometropic amblyopia. The purpose of this manipulation was to examine the feasibility of using the phase illusion as a screening test for amblyopia to distinguish it from refractive error. In experiment 2 we varied the length of the rows and the separation between the texture elements to try and understand the nature of the amblyopic impairment (Fig. 3).
The illusion was balanced by actual tilt in the opposite direction (Fig. 4). The observer indicated on each trial whether the row-pairs tapered left or right. The orientation of the rows (or envelope) was fixed at 1 of 13 preset levels to correct for the illusory tilt. The frequency of responses in the illusory direction was fitted with a cumulative normal to determine the 50% point of subjective equality, a measure of illusory tilt.
Results
Experiment 1.
There were significant differences between normal and amblyopic eyes in all three illusions (Fig. 5a). In the Fraser illusion bias was increased by amblyopia. The bias was on average greater for the amblyopes (2.72° ± 0.79° amblyopic eye, 2.08° ± 0.78° non-amblyopic eye, P < 0.05) compared with normal observers (1.71° ± 0.73°). In the phase illusion, bias was reduced by amblyopia. Amblyopes, viewing with their amblyopic eyes, saw less illusory tilt in the phase illusion (0.43° ± 0.25°) than either normal controls (0.80° ± 0.15°) or their own nonamblyopic eyes (0.74° ± 0.12°, P < 0.05). In the tilted chain illusion, the direction of the illusory tilt was reversed in three of the six amblyopic observers. Mean values were −0.06° ± 0.45° for the amblyopic eyes, versus 0.75° ± 0.16° in the non-amblyopic eye (giving P < 0.05), compared with 1.14° ± 0.12° for the normal observers. Means reported are for the core of six amblyopes who completed all three tests, and whose data are shown in Fig. 5a.
Figure 5.

Experiment 1: Comparison between amblyopic and normal illusory tilt. (a) Amblyopic and nonamblyopic illusory tilts for six amblyopes in the three illusions. Amblyopia type and depth of amblyopia are indicated for each observer (strab = strabismic, aniso = anisometropic, followed by acuity, e.g., 20/80). rj is a pure anisometrope, all others are strabismic. hc is an exception to the trends in all three illusions. Mean results of all of the amblyopes (including hc) are compared with means for six normal controls. (b) Phase illusion: data from four additional amblyopes are compared with two normal controls viewing with and without 5-diopter blur.
We tested four more amblyopes on the phase illusion, to establish whether rj was an exception in this test because his amblyopia was of the anisometropic and not the strabismic type. Of the new amblyopes three were pure anisometropes (Fig. 5b). Type of amblyopia was not predictive of responses—in all, two of the four anisometropes, and four of the six strabismics, showed a significant difference between the two eyes in the predicted direction. On average, there was a significant difference between amblyopic and nonamblyopic eyes both among the strabismic amblyopes (difference = 0.27° ± 0.25°, P < 0.05) and among the anisometropes (difference = 0.24° ± 0.23°, P < 0.05), but not between normal observers viewing with five diopters of blur and with their prescribed correction (difference = 0.12° ± 0.22°).
Best corrected acuities in the amblyopic eyes varied from mild (20/30) to moderate (20/80). Three of the four amblyopes with visual acuities of 20/50 or worse showed an effect, but only three of the six with 20/40 or better did. The size of the effect was larger in the moderate amblyopes. Depth of amblyopia might therefore be predictive of responses in this task, although the number of observers and range of amblyopia was insufficient to test the statistical significance of this trend. The single amblyopic observer (hc) who had no reduction in the tilted chain illusion was also an exception to the Fraser and phase illusions. However, another exception to the phase illusion (rj) showed a significant effect in the tilted chain.
Amblyopes suffer contrast sensitivity loss at high spatial frequencies (1). Our stimuli had high contrast (100%) and, at 3 cpd, were well within the passband of all of the amblyopes tested; in fact, most had little or no contrast sensitivity loss compared with normals at this relatively low spatial frequency. In any case, all three illusions can be seen by normal observers even with low contrast.
Experiment 2.
Decreasing the length of the rows or increasing the separation between the patches made normal performance closer to amblyopic performance (Fig. 6). The Fraser illusion was enhanced by making the rows shorter, with mean normal performance at an aspect ratio of 4:1 reaching 3.30° ± 1.12°. The phase illusion was reduced to an average of 0.56° ± 0.12° with four patches (Figs. 3a and 6a). Three of the five normal observers saw the illusion even when the patches were separated by 5 carrier periods, their average illusory tilt was 0.22° ± 0.05°. The tilted chain illusion switched direction at a row length of four patches for most normal observers (illusory tilt −0.23° ± 0.24°; Fig. 6c). Data for normal observers viewing four-tenths the row lengths used in experiment 1 were not significantly different from amblyopic data for the full row (compare results above with experiment 1).
Figure 6.

Experiment 2: Effects of row length. Gray symbols, normal controls; filled symbols, amblyopic eye of amblyopes (ae); open symbols, nonamblyopic eye of amblyopes (nae); curves, model (see text for details). All error bars show 95% confidence interval. (a) Fraser illusion. Normal data shown indicate the mean of four observers. (b) Phase illusion. Normal data are shown by a scatter from five observers. The phase illusion persisted at 5 λ separation for three of the five normal observers. (c) Tilted-chain illusion. Normal data shown indicate the mean of four observers.
We have discussed the implications of the extended spatial integration of local orientation implied by the phase illusion results elsewhere (17). We would like to point out that the reversal of the tilted-chain illusion, not previously published, as a function of decreasing row length, necessarily implies the involvement of a global mechanism in the apperception of this stimulus, as local mechanisms along the row would signal a different direction of illusion from that seen in the whole row.
Discussion
Two theories can explain the selective abnormalities in the illusory tilt seen by amblyopes. (i) The visual redundancy of the different images, as illustrated by adding the noise sources thought to occur in amblyopia, explains much (but not all) of the data (Fig. 2). (ii) Amblyopic performance was also close to normal performance with shorter rows, implying a dominance of local over global information or perhaps a failure to integrate local signals into a more global structure (Fig. 3).
The images in Fig. 2 have been undersampled, and both the phase and the location of the patches has been jittered. These manipulations demonstrate the reduction in the phase illusion caused by noisy image degradation, and the reversal of the tilted chain, but there is no increase in the Fraser illusion. Psychophysical data show that amblyopes are particularly poor at relative phase judgements (7, 8) and, clearly, complete phase randomization would eradicate the phase illusion. However, although there is neurophysiological evidence of spatial undersampling in the primary visual cortex of amblyopic monkeys, there is as yet no evidence of topographical jitter (which is necessary to alter the tilt illusions) in the filter mosaic of amblyopic monkeys (2). For these reasons, we sought a higher level explanation of our findings.
Fraser (12) suggested that “There are possibly present as factors in the illusion two distinct visual integrative processes: (a) One corresponding to a line joining the centres of areas of the units. This may be looked on as a form of confluent union. (b) One representing collectively the trends or tendencies of the units.” This idea has been used to explain the Fraser illusion, in neurophysiological terms, as the integration of orientation units (or linear filters) by second order (nonlinear) collator mechanisms (14, 18) or cortical interactions (19). The model data in Fig. 6 show a simple application of this theory to the stimuli. Stimuli were filtered with elongated Gabor filters (20) (σ = 2λ), and the distribution of activity across orientations was convolved with a Gaussian (0.5° ≤ σ ≤ 5°) centered on horizontal to model the envelope orientation signal. (The envelope orientation is the axis of elongation of the stimulus patch in the Fraser illusion, or the orientation of the line joining the centers of the patches in the phase and tilted-chain illusions. This is equivalent in Fraser's terminology to the line joining the centers of the units.) Results show weighted mean orientation in this filter bank.
Our findings could be explained if the amblyopes simply fail to integrate visual information along the full length of the rows. In all three illusions, amblyopes perform like normal observers would given shorter rows (Fig. 3). Unlike the more general image degradation seen in Fig. 2, this finding can also account for the enhanced Fraser illusion seen by amblyopes. A failure to integrate visual stimuli across space could also explain other deficits of amblyopes, which cannot be explained by their contrast sensitivity loss or by undersampling. These include reduced visual acuity (1), the absence of Vernier hyperacuity (3), impaired contour detection in noise (21), raised jitter detection thresholds (22), and the undercounting of spatially distributed visual stimuli (23). All these tasks require visual integration across space. Unevenly distributed impairments in spatial integration (due, perhaps, to local undersampling) may give the psychophysical appearance of topographical jitter, resulting in the localization biases observed in some strabismic amblyopes (1). Although most of our results are consistent with the idea of topographical jitter, a more cogent explanation can be found in terms of a higher order deficit of spatial integration.
In summary, possible explanations for the altered illusory perceptions of the amblyopes are: (i) visual noise and (ii) dominance of local over global signals.
The results presented in this paper make a number of important contributions to visual science. They demonstrate the extent of grouping or interaction across the visual field in normal human observers, where illusory tilt increased up to a row length of about 10° (or 40 carrier periods). They suggest that, in addition to models based on different sources of visual noise, some of the impairment in amblyopia may be the result of impaired grouping processes. The demonstration of significant differences between the biases obtained in normal and amblyopic eyes, which are not simply the result of poor visibility, offers hope of a positive diagnostic test which can distinguish between amblyopia and uncorrected refractive error. Amblyopia is currently diagnosed by exclusion (i.e., the elimination of organic disease and refractive error, which is often difficult to measure accurately in preliterate children). Amblyopia can be treated by occlusion therapy, which is thought to encourage the development of visual pathways in the brain associated with the amblyopic eye (1), with adult amblyopes demonstrating significant neural plasticity (24). The illusion images could be used for screening young children for the disorder and for monitoring the effects of treatment.
Acknowledgments
This work was supported by Grants R01EY01728 and P30EY07551 from the National Eye Institute (National Institutes of Health).
Footnotes
This paper was submitted directly (Track II) to the PNAS office.
References
- 1.Ciuffreda K J, Levi D M, Selenow A. Amblyopia, Basic and Clinical Aspects. Boston: Butterworth-Heinemann; 1991. [Google Scholar]
- 2.Kiorpes L, McKee S P. Curr Opin Neurobiol. 1999;4:480–486. doi: 10.1016/s0959-4388(99)80072-5. [DOI] [PubMed] [Google Scholar]
- 3.Levi D M, Klein S A. Vision Res. 1985;25:979–991. doi: 10.1016/0042-6989(85)90208-1. [DOI] [PubMed] [Google Scholar]
- 4.Wilson H R. Vision Res. 1991;31:967–982. doi: 10.1016/0042-6989(91)90204-i. [DOI] [PubMed] [Google Scholar]
- 5.Sharma V, Levi D M, Coletta N J. Vision Res. 1999;39:3526–3536. doi: 10.1016/s0042-6989(99)00028-0. [DOI] [PubMed] [Google Scholar]
- 6.Hess R F, Campbell F W, Greenhalgh T. Pflügers Arch. 1978;377:201–207. doi: 10.1007/BF00584273. [DOI] [PubMed] [Google Scholar]
- 7.Lawden M C, Hess R F, Campbell F W. Vision Res. 1982;22:1005–1016. doi: 10.1016/0042-6989(82)90037-2. [DOI] [PubMed] [Google Scholar]
- 8.Pass A F, Levi D M. Invest Ophthalmol Visual Sci. 1982;23:780–786. [PubMed] [Google Scholar]
- 9.Morgan M J. Vision Res. 1999;39:2361–2380. doi: 10.1016/s0042-6989(98)00243-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Morgan M J, Hole G J, Glennerster A. Vision Res. 1990;30:1793–1810. doi: 10.1016/0042-6989(90)90160-m. [DOI] [PubMed] [Google Scholar]
- 11.Warrington E K, Taylor A M. Perception. 1978;7:695–705. doi: 10.1068/p070695. [DOI] [PubMed] [Google Scholar]
- 12.Fraser J. Br J Psychol. 1908;2:307–320. [Google Scholar]
- 13.Ohzawa I, DeAngelis G C, Freeman R D. J Neurophysiol. 1996;75:1779–1805. doi: 10.1152/jn.1996.75.5.1779. [DOI] [PubMed] [Google Scholar]
- 14.Morgan M J, Baldassi S. Curr Biol. 1997;7:999–1002. doi: 10.1016/s0960-9822(06)00421-0. [DOI] [PubMed] [Google Scholar]
- 15.Popple A V, Sagi D. Vision Res. 2000;40:873–878. doi: 10.1016/s0042-6989(00)00010-9. [DOI] [PubMed] [Google Scholar]
- 16.Stuart G W, Day R H. Percept Psychophys. 1988;44:409–420. doi: 10.3758/bf03210425. [DOI] [PubMed] [Google Scholar]
- 17.Popple A V, Levi D M. Vision Res. 2000;40:2545–2549. doi: 10.1016/s0042-6989(00)00127-9. [DOI] [PubMed] [Google Scholar]
- 18.Morgan M, Castet E, Ward R. Q J Exp Psychol. 1998;51:347–371. doi: 10.1080/713755766. [DOI] [PubMed] [Google Scholar]
- 19.Polat U, Tyler C W. Vision Res. 1999;39:887–895. doi: 10.1016/s0042-6989(98)00245-4. [DOI] [PubMed] [Google Scholar]
- 20.Geisler W S, Albrecht D G. Visual Neurosci. 1997;14:897–919. doi: 10.1017/s0952523800011627. [DOI] [PubMed] [Google Scholar]
- 21.Hess R F, McIlhagga W, Field D J. Vision Res. 1997;37:3145–3161. doi: 10.1016/s0042-6989(96)00281-7. [DOI] [PubMed] [Google Scholar]
- 22.Levi D M, Klein S A, Sharma V. Vision Res. 1999;39:445–465. doi: 10.1016/s0042-6989(98)00125-4. [DOI] [PubMed] [Google Scholar]
- 23.Sharma V, Levi D M, Klein S A. Nat Neurosci. 2000;5:496–501. doi: 10.1038/74872. [DOI] [PubMed] [Google Scholar]
- 24.Levi D M, Polat U. Proc Natl Acad Sci USA. 1996;93:6830–6834. doi: 10.1073/pnas.93.13.6830. [DOI] [PMC free article] [PubMed] [Google Scholar]