

Abstract
BACKGROUND—Some patients with faecal incontinence are not amenable to simple surgical sphincter repair, due to sphincter weakness in the absence of a structural defect. AIMS—To evaluate the efficacy and possible mode of action of short term stimulation of sacral nerves in patients with faecal incontinence and a structurally intact external anal sphincter. PATIENTS—Twelve patients with faecal incontinence for solid or liquid stool at least once per week. METHODS—A stimulating electrode was placed (percutaneously in 10 patients, operatively in two) into the S3 or S4 foramen. The electrode was left in situ for a minimum of one week with chronic stimulation. RESULTS—Evaluable results were obtained in nine patients, with early electrode displacement in the other three. Incontinence ceased in seven of nine patients and improved notably in one; one patient with previous imperforate anus and sacral agenesis had no symptomatic response. Stimulation seemed to enhance maximum squeeze pressure but did not alter resting pressure. The rectum became less sensitive to distension with no change in rectal compliance. Ambulatory studies showed a possible reduction in rectal contractile activity and diminished episodes of spontaneous anal relaxation. CONCLUSIONS—Short term sacral nerve stimulation notably decreases episodes of faecal incontinence. The effect may be mediated via facilitation of striated sphincter muscle function, and via neuromodulation of sacral reflexes which regulate rectal sensitivity and contractility, and anal motility.
Keywords: sacral nerve stimulation; faecal incontinence
Full Text
The Full Text of this article is available as a PDF (141.5 KB).
Figure 1 .
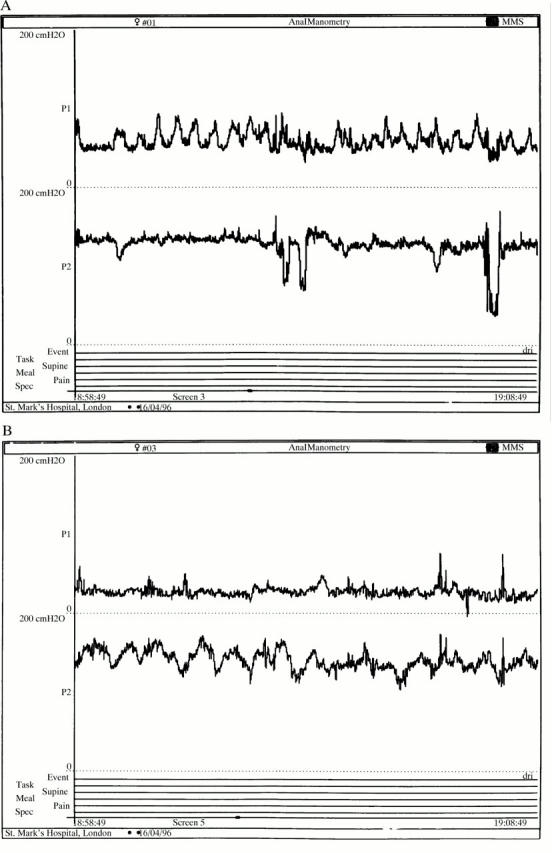
Ten minute traces from the 24 hour ambulatory studies of patient FH. (A) Before stimulation; (B) after stimulation. The upper trace shows rectal activity and the lower trace anal activity. Stimulation seems to reduce rectal contractile activity and to cause qualitative changes in anal contractile activity with induction of slow wave activity and a reduction in transient relaxations.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Baeten C. G., Geerdes B. P., Adang E. M., Heineman E., Konsten J., Engel G. L., Kester A. D., Spaans F., Soeters P. B. Anal dynamic graciloplasty in the treatment of intractable fecal incontinence. N Engl J Med. 1995 Jun 15;332(24):1600–1605. doi: 10.1056/NEJM199506153322403. [DOI] [PubMed] [Google Scholar]
- Bosch J. L., Groen J. Sacral (S3) segmental nerve stimulation as a treatment for urge incontinence in patients with detrusor instability: results of chronic electrical stimulation using an implantable neural prosthesis. J Urol. 1995 Aug;154(2 Pt 1):504–507. doi: 10.1097/00005392-199508000-00045. [DOI] [PubMed] [Google Scholar]
- Browning G. G., Motson R. W. Results of Parks operation for faecal incontinence after anal sphincter injury. Br Med J (Clin Res Ed) 1983 Jun 11;286(6381):1873–1875. doi: 10.1136/bmj.286.6381.1873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Engel A. F., Kamm M. A., Bartram C. I., Nicholls R. J. Relationship of symptoms in faecal incontinence to specific sphincter abnormalities. Int J Colorectal Dis. 1995;10(3):152–155. doi: 10.1007/BF00298538. [DOI] [PubMed] [Google Scholar]
- Engel A. F., Kamm M. A., Sultan A. H., Bartram C. I., Nicholls R. J. Anterior anal sphincter repair in patients with obstetric trauma. Br J Surg. 1994 Aug;81(8):1231–1234. doi: 10.1002/bjs.1800810853. [DOI] [PubMed] [Google Scholar]
- Engel A. F., Kamm M. A., Talbot I. C. Progressive systemic sclerosis of the internal anal sphincter leading to passive faecal incontinence. Gut. 1994 Jun;35(6):857–859. doi: 10.1136/gut.35.6.857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Habib H. N. Experience and recent contributions in sacral nerve stimulation for voiding in both human and animal. Br J Urol. 1967 Feb;39(1):73–83. doi: 10.1111/j.1464-410x.1967.tb11787.x. [DOI] [PubMed] [Google Scholar]
- Jorge J. M., Wexner S. D. Anorectal manometry: techniques and clinical applications. South Med J. 1993 Aug;86(8):924–931. doi: 10.1097/00007611-199308000-00016. [DOI] [PubMed] [Google Scholar]
- Kamm M. A., Lennard-Jones J. E. Rectal mucosal electrosensory testing--evidence for a rectal sensory neuropathy in idiopathic constipation. Dis Colon Rectum. 1990 May;33(5):419–423. doi: 10.1007/BF02156270. [DOI] [PubMed] [Google Scholar]
- Kiff E. S., Swash M. Slowed conduction in the pudendal nerves in idiopathic (neurogenic) faecal incontinence. Br J Surg. 1984 Aug;71(8):614–616. doi: 10.1002/bjs.1800710817. [DOI] [PubMed] [Google Scholar]
- Lehur P. A., Michot F., Denis P., Grise P., Leborgne J., Teniere P., Buzelin J. M. Results of artificial sphincter in severe anal incontinence. Report of 14 consecutive implantations. Dis Colon Rectum. 1996 Dec;39(12):1352–1355. doi: 10.1007/BF02054523. [DOI] [PubMed] [Google Scholar]
- Lembo T., Munakata J., Mertz H., Niazi N., Kodner A., Nikas V., Mayer E. A. Evidence for the hypersensitivity of lumbar splanchnic afferents in irritable bowel syndrome. Gastroenterology. 1994 Dec;107(6):1686–1696. doi: 10.1016/0016-5085(94)90809-5. [DOI] [PubMed] [Google Scholar]
- Matzel K. E., Stadelmaier U., Hohenfellner M., Gall F. P. Electrical stimulation of sacral spinal nerves for treatment of faecal incontinence. Lancet. 1995 Oct 28;346(8983):1124–1127. doi: 10.1016/s0140-6736(95)91799-3. [DOI] [PubMed] [Google Scholar]
- Neill M. E., Parks A. G., Swash M. Physiological studies of the anal sphincter musculature in faecal incontinence and rectal prolapse. Br J Surg. 1981 Aug;68(8):531–536. doi: 10.1002/bjs.1800680804. [DOI] [PubMed] [Google Scholar]
- Nielsen M. B., Hauge C., Rasmussen O. O., Pedersen J. F., Christiansen J. Anal endosonographic findings in the follow-up of primarily sutured sphincteric ruptures. Br J Surg. 1992 Feb;79(2):104–106. doi: 10.1002/bjs.1800790204. [DOI] [PubMed] [Google Scholar]
- Peña A. Current management of anorectal anomalies. Surg Clin North Am. 1992 Dec;72(6):1393–1416. doi: 10.1016/s0039-6109(16)45887-1. [DOI] [PubMed] [Google Scholar]
- Speakman C. T., Kamm M. A. The internal and sphincter--new insights into faecal incontinence. Gut. 1991 Apr;32(4):345–346. doi: 10.1136/gut.32.4.345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vaizey C. J., Kamm M. A., Bartram C. I. Primary degeneration of the internal anal sphincter as a cause of passive faecal incontinence. Lancet. 1997 Mar 1;349(9052):612–615. doi: 10.1016/S0140-6736(96)09188-X. [DOI] [PubMed] [Google Scholar]