

Abstract
OBJECTIVE—To clarify the usefulness of endoscopic ultrasonography (EUS) and endoscopy in the endoscopic mucosal resection (EMR) of early gastric cancer. Patients/Methods—EMR was performed in 61 patients with early gastric cancer over the past five years. The accuracy of the assessment of the depth of cancerous invasion was studied in 49 patients who had EUS before EMR. Forty eight patients were treated with endoscopy alone; in these patients, EUS and endoscopic findings correlated with the clinical course. RESULTS—Forty six patients showed no changes in the submucosal layer or deeper structures on EUS. Pathologically these included 37 patients with mucosal cancer and nine with submucosal cancer showing very slight submucosal infiltration. Three patients showed diffuse low echo changes in the submucosal layer on EUS; pathologically, these included two with submucosal cancer and one with mucosal cancer with a peptic ulcer scar within the tumour focus. Of 48 patients receiving endoscopic treatment alone, 45 showed no tumour recurrence or evidence of metastases on EUS and endoscopy. Three cases of recurrence were observed. Two of these patients had a surgical gastrectomy, and one was re-treated endoscopically. In the former cases, the surgical results correlated well with assessment by EUS and endoscopy. In addition, the latter patient who was re-treated endoscopically after evaluation with EUS and endoscopy has so far had no recurrence. CONCLUSION—The combined use of EUS and endoscopy is effective in diagnosing the depth of cancerous invasion in patients undergoing EMR as well as in clarifying changes both within and between anatomic levels during follow up. Keywords: endoscopic ultrasonography; endoscopy; mucosal resection; gastric cancer
Full Text
The Full Text of this article is available as a PDF (223.9 KB).
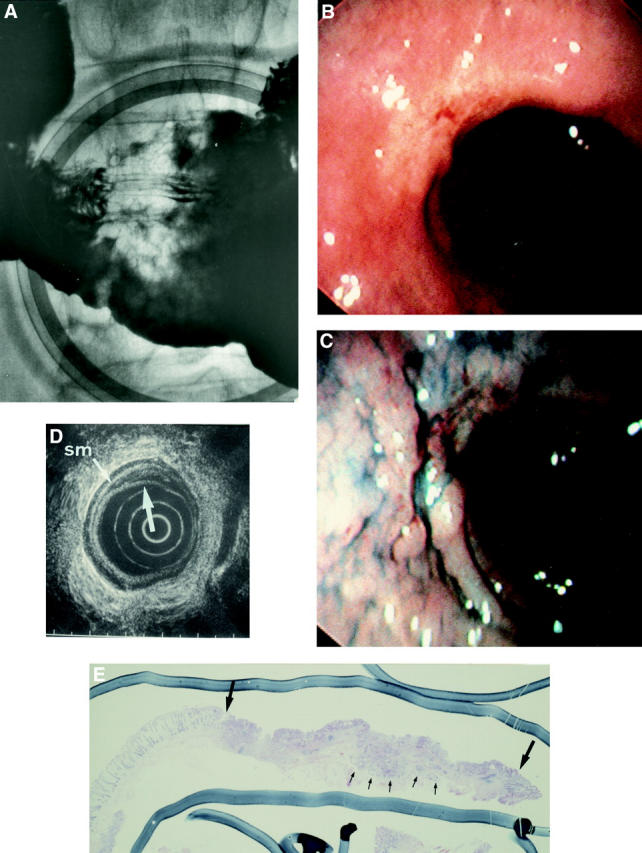
Figure 1 .

A group A patient with mucosal cancer, a negative stump, and no ulcer in the tumour focus at endoscopic one step resection. Type IIc early cancer before endoscopic resection. (A) Normal endoscopic picture; (B) indigo carmine spray endoscopic picture; (C) double contrast radiograph; (D) endoscopic ultrasonography showing no change in the submucosal layer or deeper.
Figure 2 .

One year after endoscopic mucosal resection. (A) Endoscopic picture showing s1 scar; (B) endoscopic ultrasonography shows Ul-IIs changes resembling benign ulcer. No lymphadenopathy is observed.
Figure 3 .

Three years and one month after endoscopic mucosal resection. Endoscopic ultrasonography shows Ul-IIs changes resembling benign ulcer. No lymphadenopathy is observed. sm, submucosal.
Figure 4 .

Three years and nine months after endoscopic mucosal resection. Endoscopic picture showing s2 scar.
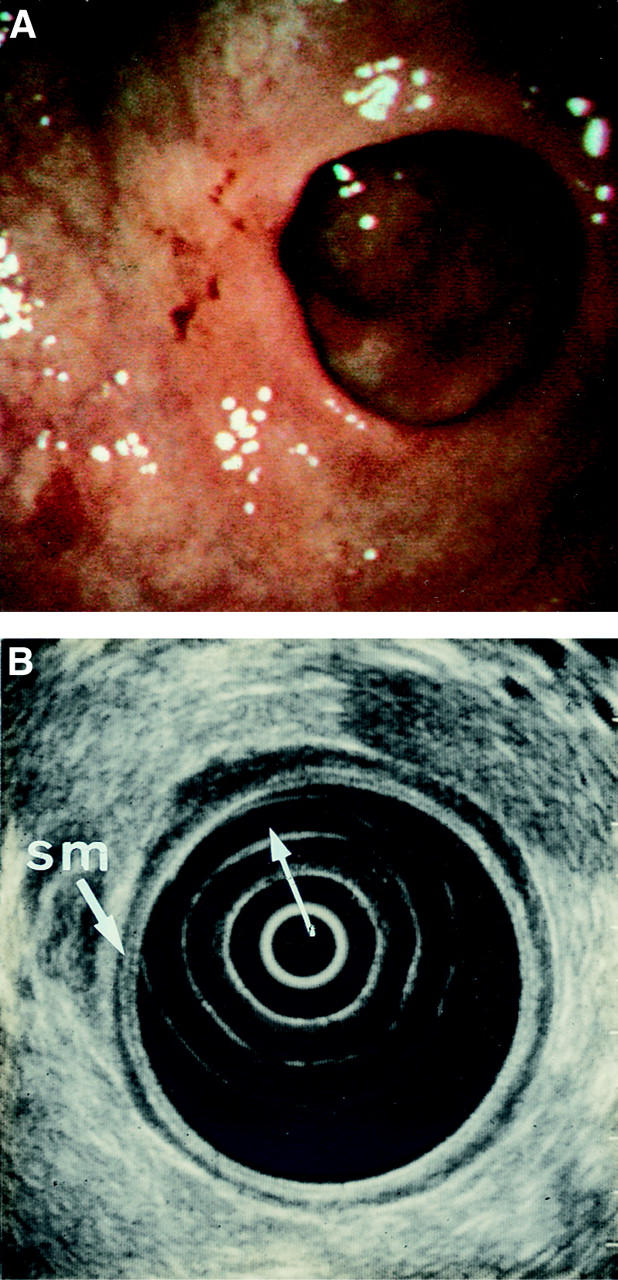
Figure 5 .
A group C patient with submucosal cancer (slight invasion of submucosa) showing a negative stump at endoscopic piecemeal resection. He refused surgery (recurrent; fig 9C). (A) Double contrast radiograph; (B) normal endoscopic picture; (C) indigo carmine spray endoscopic picture; (D) endoscopic ultrasonography shows no change in the submucosal (sm) layer or deeper; (E) a cross section.
Figure 6 .
One year after endoscopic mucosal resection. Endoscopic picture showing s2 scar. Biopsy specimen gave negative results for cancer.
Figure 7 .
Two years after endoscopic mucosal resection. (A) Endoscopic picture showing s2 scar-like appearance. Biopsy specimen gave positive results for cancer. (B) Endoscopic ultrasonography shows Ul-IIs changes resembling benign ulcer. No lymphadenopathy is observed. sm, submucosal.
Figure 8 .

Two years and nine months after endoscopic mucosal resection and seven months after endoscopic combined treatment (laser and pure ethanol injection). Endoscopic picture showing s2 scar. A biopsy specimen gave negative results for cancer.
Figure 9 .

Endoscopic ultrasonography (EUS), endoscopic, and histological findings for three patients with recurrence of gastric cancer after endoscopic mucosal resection (EMR). Ul-IIs on EUS, ulcer scar image resembling benign ulcer and no tumour invasion or ultrasonographic changes.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aibe T., Fuji T., Okita K., Takemoto T. A fundamental study of normal layer structure of the gastrointestinal wall visualized by endoscopic ultrasonography. Scand J Gastroenterol Suppl. 1986;123:6–15. doi: 10.3109/00365528609091857. [DOI] [PubMed] [Google Scholar]
- Hirao M., Masuda K., Asanuma T., Naka H., Noda K., Matsuura K., Yamaguchi O., Ueda N. Endoscopic resection of early gastric cancer and other tumors with local injection of hypertonic saline-epinephrine. Gastrointest Endosc. 1988 May-Jun;34(3):264–269. doi: 10.1016/s0016-5107(88)71327-9. [DOI] [PubMed] [Google Scholar]
- Hole D. J., Quigley E. M., Gillis C. R., Watkinson G. Peptic ulcer and cancer: an examination of the relationship between chronic peptic ulcer and gastric carcinoma. Scand J Gastroenterol. 1987 Jan;22(1):17–23. doi: 10.3109/00365528708991850. [DOI] [PubMed] [Google Scholar]
- Karita M., Tada M., Okita K. The successive strip biopsy partial resection technique for large early gastric and colon cancers. Gastrointest Endosc. 1992 Mar-Apr;38(2):174–178. doi: 10.1016/s0016-5107(92)70386-1. [DOI] [PubMed] [Google Scholar]
- Lambert R. Curative endoscopic treatment of early esophageal and gastric cancer. Bildgebung. 1993 Apr;60 (Suppl 1):8–12. [PubMed] [Google Scholar]
- Niwa Y., Nakazawa S., Yoshino J., Nakamura T., Ohashi S., Tsukamoto Y. Quantification of gastric ulcer healing by endoscopic ultrasonography. Gastrointest Endosc. 1990 Mar-Apr;36(2):116–122. doi: 10.1016/s0016-5107(90)70963-7. [DOI] [PubMed] [Google Scholar]
- Ohashi S., Nakazawa S., Yoshino J. Endoscopic ultrasonography in the assessment of invasive gastric cancer. Scand J Gastroenterol. 1989 Nov;24(9):1039–1048. doi: 10.3109/00365528909089253. [DOI] [PubMed] [Google Scholar]
- Takekoshi T., Baba Y., Ota H., Kato Y., Yanagisawa A., Takagi K., Noguchi Y. Endoscopic resection of early gastric carcinoma: results of a retrospective analysis of 308 cases. Endoscopy. 1994 May;26(4):352–358. doi: 10.1055/s-2007-1008990. [DOI] [PubMed] [Google Scholar]
- Tio T. L., Tytgat G. N. Endoscopic ultrasonography in the assessment of intra- and transmural infiltration of tumours in the oesophagus, stomach and papilla of Vater and in the detection of extraoesophageal lesions. Endoscopy. 1984 Nov;16(6):203–210. doi: 10.1055/s-2007-1018581. [DOI] [PubMed] [Google Scholar]