

Abstract
BACKGROUND—The common but incompletely understood entity of malabsorption of food bound cobalamin is generally presumed to arise from gastritis and/or achlorhydria. AIM—To conduct a systematic comparative examination of gastric histology and function. SUBJECTS—Nineteen volunteers, either healthy or with low cobalamin levels, were prospectively studied without prior knowledge of their absorption or gastric status. METHODS—All subjects underwent prospective assessment of food cobalamin absorption by the egg yolk cobalamin absorption test, endoscopy, histological grading of biopsies from six gastric sites, measurement of gastric secretory function, assay for serum gastrin and antiparietal cell antibodies, and direct tests for Helicobacter pylori infection. RESULTS—The six subjects with severe malabsorption (group I) had worse histological scores overall and lower acid and pepsin secretion than the eight subjects with normal absorption (group III) or the five subjects with mild malabsorption (group II). However, histological findings, and acid and pepsin secretion overlapped considerably between individual subjects in group I and group III. Two distinct subgroups of three subjects each emerged within group I. One subgroup (IA) had severe gastric atrophy and achlorhydria. The other subgroup (IB) had little atrophy and only mild hypochlorhydria; the gastric findings were indistinguishable from those in many subjects with normal absorption. Absorption improved in the two subjects in subgroup IB and in one subject in group II who received antibiotics, along with evidence of clearing of H pylori. None of the subjects in group IA responded to antibiotics. CONCLUSIONS—Food cobalamin malabsorption arises in at least two different gastric settings, one of which involves neither gastric atrophy nor achlorhydria. Malabsorption can respond to antibiotics, but only in some patients. Food cobalamin malabsorption is not always synonymous with atrophic gastritis and achlorhydria, and hypochlorhydria does not always guarantee food cobalamin malabsorption. Keywords: cobalamin; cobalamin malabsorption; atrophic gastritis; achlorhydria; pepsin; gastrin; Helicobacter pylori
Full Text
The Full Text of this article is available as a PDF (278.9 KB).
Figure 1 .

Diagrammatic representation of the gastric biopsy sites.
Figure 2 .

Low power view of a normal appearing oxyntic biopsy from the mid body greater curvature from subject No 14 in group III. Note that the pits (P) are close together (arrow), not separated as in figure 4 by inflammatory cells. The band of predominantly red staining cells below the pits is where parietal cells are concentrated. The predominantly blue staining gland zone beneath that band is where chief cells are concentrated.
Figure 3 .

Severe atrophic gastritis of the mid body greater curvature in subject No 2 in subgroup IA with severe food cobalamin malabsorption. Most of the section shows full thickness intestinal metaplasia with villi lined by enterocytes and goblet cells. The centre is lined by gastric surface epithelium and, beneath it, a small group of residual glands. The clear staining glands (thin arrow) are metaplastic mucous glands (pseudopyloric metaplasia). The blue and red cells in the centre are chief and parietal cells (thick arrow).
Figure 4 .

Mid body biopsy from subject No 6 in subgroup IB. A dense infiltrate separates the gastric pits (contrast with fig 2). There is encroachment of inflammatory cells beneath the pits into the uppermost part of the gland zone. This was graded as mild atrophic gastritis. It could be argued, however, that this is the severe end of the superficial gastritis spectrum, which would only strengthen the concept that severe malabsorption occurs in the absence of atrophy.
Figure 5 .
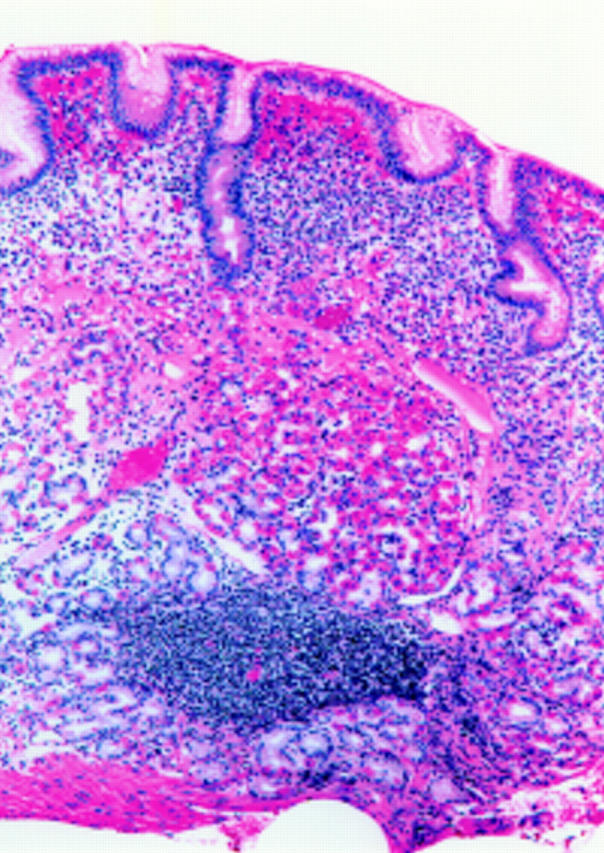
Biopsy from the mid body in subject No 10 from group II with mild food cobalamin malabsorption. Inflammatory cells separate the pits, similar to fig 4. A plug of oxyntic glands sits atop a lymphoid aggregate. To the left is pink staining oedema fluid.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Carmel R., Green R., Jacobsen D. W., Rasmussen K., Florea M., Azen C. Serum cobalamin, homocysteine, and methylmalonic acid concentrations in a multiethnic elderly population: ethnic and sex differences in cobalamin and metabolite abnormalities. Am J Clin Nutr. 1999 Nov;70(5):904–910. doi: 10.1093/ajcn/70.5.904. [DOI] [PubMed] [Google Scholar]
- Carmel R. In vitro studies of gastric juice in patients with food-cobalamin malabsorption. Dig Dis Sci. 1994 Dec;39(12):2516–2522. doi: 10.1007/BF02087684. [DOI] [PubMed] [Google Scholar]
- Carmel R., Perez-Perez G. I., Blaser M. J. Helicobacter pylori infection and food-cobalamin malabsorption. Dig Dis Sci. 1994 Feb;39(2):309–314. doi: 10.1007/BF02090202. [DOI] [PubMed] [Google Scholar]
- Carmel R., Sinow R. M., Siegel M. E., Samloff I. M. Food cobalamin malabsorption occurs frequently in patients with unexplained low serum cobalamin levels. Arch Intern Med. 1988 Aug;148(8):1715–1719. [PubMed] [Google Scholar]
- Dawson D. W., Sawers A. H., Sharma R. K. Malabsorption of protein bound vitamin B12. Br Med J (Clin Res Ed) 1984 Mar 3;288(6418):675–678. doi: 10.1136/bmj.288.6418.675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Del Corral A., Carmel R. Transfer of cobalamin from the cobalamin-binding protein of egg yolk to R binder of human saliva and gastric juice. Gastroenterology. 1990 Jun;98(6):1460–1466. doi: 10.1016/0016-5085(90)91076-i. [DOI] [PubMed] [Google Scholar]
- Doscherholmen A., Silvis S., McMahon J. Dual isotope Schilling test for measuring absorption of food-bound and free vitamin B12 simultaneously. Am J Clin Pathol. 1983 Oct;80(4):490–495. doi: 10.1093/ajcp/80.4.490. [DOI] [PubMed] [Google Scholar]
- Doscherholmen A., Swaim W. R. Impaired assimilation of egg Co 57 vitamin B 12 in patients with hypochlorhydria and achlorhydria and after gastric resection. Gastroenterology. 1973 May;64(5):913–919. [PubMed] [Google Scholar]
- GOTTLIEBLAU K. S., WASSERMAN L. R., HERBERT V. RAPID CHARCOAL ASSAY FOR INTRINSIC FACTOR (IF), GASTRIC JUICE UNSATURATED B12 BINDING CAPACITY, ANTIBODY TO IF, AND SERUM UNSATURATED B12 BINDING CAPACITY. Blood. 1965 Jun;25:875–884. [PubMed] [Google Scholar]
- Genta R. M., Robason G. O., Graham D. Y. Simultaneous visualization of Helicobacter pylori and gastric morphology: a new stain. Hum Pathol. 1994 Mar;25(3):221–226. doi: 10.1016/0046-8177(94)90191-0. [DOI] [PubMed] [Google Scholar]
- Gutierrez O., Melo M., Segura A. M., Angel A., Genta R. M., Graham D. Y. Cure of Helicobacter pylori infection improves gastric acid secretion in patients with corpus gastritis. Scand J Gastroenterol. 1997 Jul;32(7):664–668. doi: 10.3109/00365529708996515. [DOI] [PubMed] [Google Scholar]
- Laine L., Marin-Sorensen M., Weinstein W. M. Nonsteroidal antiinflammatory drug-associated gastric ulcers do not require Helicobacter pylori for their development. Am J Gastroenterol. 1992 Oct;87(10):1398–1402. [PubMed] [Google Scholar]
- Lindgren A., Bagge E., Cederblad A., Nilsson O., Persson H., Kilander A. F. Schilling and protein-bound cobalamin absorption tests are poor instruments for diagnosing cobalamin malabsorption. J Intern Med. 1997 Jun;241(6):477–484. doi: 10.1111/j.1365-2796.1997.tb00005.x. [DOI] [PubMed] [Google Scholar]
- Marcuard S. P., Albernaz L., Khazanie P. G. Omeprazole therapy causes malabsorption of cyanocobalamin (vitamin B12) Ann Intern Med. 1994 Feb 1;120(3):211–215. doi: 10.7326/0003-4819-120-3-199402010-00006. [DOI] [PubMed] [Google Scholar]
- Miller A., Slingerland D. W., Hall C. A., Chu R. C. Food-bound B12 absorption and serum total homocysteine in patients with low serum B12 levels. Am J Hematol. 1998 Sep;59(1):42–45. doi: 10.1002/(sici)1096-8652(199809)59:1<42::aid-ajh8>3.0.co;2-#. [DOI] [PubMed] [Google Scholar]
- Saltzman J. R., Kemp J. A., Golner B. B., Pedrosa M. C., Dallal G. E., Russell R. M. Effect of hypochlorhydria due to omeprazole treatment or atrophic gastritis on protein-bound vitamin B12 absorption. J Am Coll Nutr. 1994 Dec;13(6):584–591. doi: 10.1080/07315724.1994.10718452. [DOI] [PubMed] [Google Scholar]
- Skak-Nielsen T., Holst J. J., Nielsen O. V. Role of gastrin-releasing peptide in the neural control of pepsinogen secretion from the pig stomach. Gastroenterology. 1988 Nov;95(5):1216–1220. doi: 10.1016/0016-5085(88)90353-8. [DOI] [PubMed] [Google Scholar]
- Steinberg W. M., King C. E., Toskes P. P. Malabsorption of protein-bound cobalamin but not unbound cobalamin during cimetidine administration. Dig Dis Sci. 1980 Mar;25(3):188–191. doi: 10.1007/BF01308137. [DOI] [PubMed] [Google Scholar]
- Streeter A. M., Duraiappah B., Boyle R., O'Neill B. J., Pheils M. T. Malabsorption of vitamin B12 after vagotomy. Am J Surg. 1974 Sep;128(3):340–343. doi: 10.1016/0002-9610(74)90169-x. [DOI] [PubMed] [Google Scholar]
- Suter P. M., Golner B. B., Goldin B. R., Morrow F. D., Russell R. M. Reversal of protein-bound vitamin B12 malabsorption with antibiotics in atrophic gastritis. Gastroenterology. 1991 Oct;101(4):1039–1045. doi: 10.1016/0016-5085(91)90731-y. [DOI] [PubMed] [Google Scholar]
- van Asselt D. Z., de Groot L. C., van Staveren W. A., Blom H. J., Wevers R. A., Biemond I., Hoefnagels W. H. Role of cobalamin intake and atrophic gastritis in mild cobalamin deficiency in older Dutch subjects. Am J Clin Nutr. 1998 Aug;68(2):328–334. doi: 10.1093/ajcn/68.2.328. [DOI] [PubMed] [Google Scholar]