

Abstract
OBJECTIVE—To determine the long term outcome in patients treated with percutaneous transluminal septal myocardial ablation (PTSMA) for hypertrophic obstructive cardiomyopathy (HOCM). DESIGN AND SETTING—Observational, single centre study. PATIENTS—25 patients (13 women, 12 men, mean (SD) age 54.7 (15.0) years) with drug treatment resistant New York Heart Association (NYHA) class 2.8 (0.6) symptoms attributed to a high left ventricular outflow gradient (LVOTG) and a coronary artery anatomy suitable for intervention. INTERVENTION—PTSMA by injection of 4.1 (2.6) ml of alcohol (96%) into 1.4 (0.6) septal perforator arteries to ablate the hypertrophied interventricular septum. OUTCOME MEASURES—During in-hospital follow up, enzyme rise, the frequency of atrioventricular conduction lesions requiring permanent DDD pacing, and in-hospital mortality were assessed. Long term follow up (30 (4) months, range 24-36 months) included symptoms, echocardiographic measurements of left atrial and left ventricular dimensions and function, and LVOTG. RESULTS—Mean postinterventional creatine kinase rise was 780 (436) U/l. During PTSMA 13 patents developed total heart block, permanent pacing being necessary in five of them. One 86 year old patient died from ventricular fibrillation associated with intensive treatment (β mimetic and theophylline) for coexistent severe obstructive airway disease. After three months, three patients underwent re-PTSMA because of a dissatisfactory primary result, leading to LVOTG elimination in all of them. During long term follow up, LVOTG showed sustained reduction (3 (6) mm Hg at rest and 12 (19) mm Hg with provocation) associated with stable symptomatic improvement (NYHA class 1.2 (1.0)) and without significant global left ventricular dilatation. CONCLUSIONS—PTSMA is an effective non-surgical technique for reduction of symptoms and LVOTG in HOCM. Prospective, long term observations of larger populations are necessary in order to determine the definitive significance of the procedure. Keywords: hypertrophic obstructive cardiomyopathy; percutaneous transluminal septal myocardial ablation; left ventricular outflow tract gradient; myocardial contrast echocardiography
Full Text
The Full Text of this article is available as a PDF (175.2 KB).
Figure 1 .
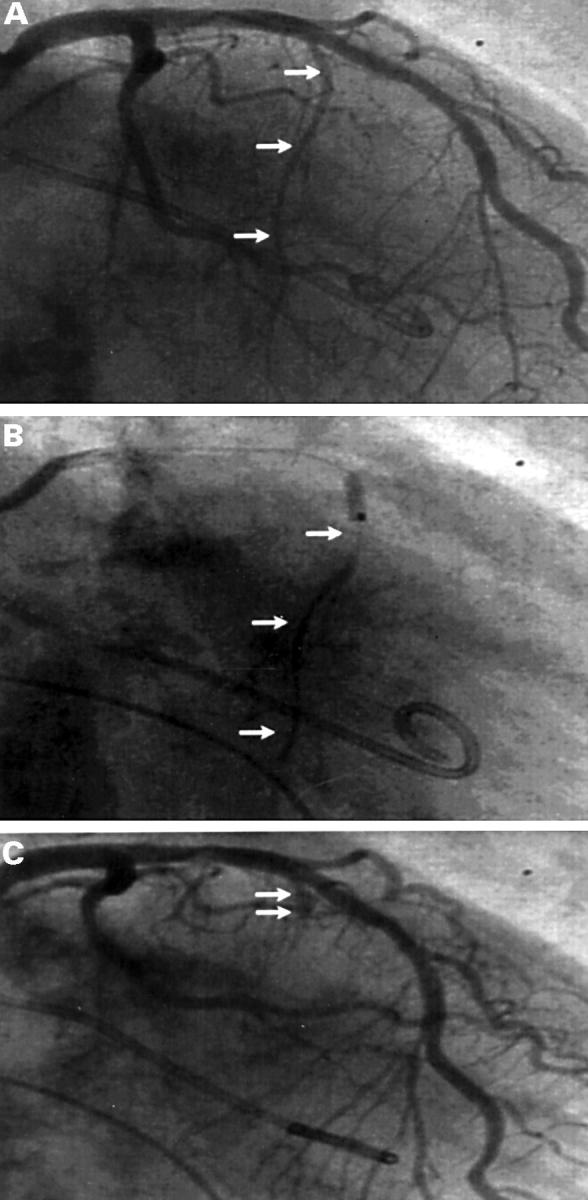
Coronary angiograms. (A) Identification of the target vessel in right anterior oblique position (arrows). (B) Injection of contrast dye to define the perfusion area and to exclude reflux into the left anterior descending coronary artery. (C) Final visualisation of the vessel stump after completed PTSMA.
Figure 2 .

Haemodynamic treatment result of PTSMA. Pressure curves of left ventricular inflow tract (LV) and aorta (AO) before (left) and after (right) intervention with complete elimination of the LVOTG and reduction of left ventricular end diastolic pressure (lower arrows).
Figure 3 .

Morphological results of PTSMA. Parasternal long axis view (A) and apical four chamber view (B) before (left) and after (right) PTSMA, showing the myectomy like subaortic scar leading to widening of the LVOT. Posterior wall of the left ventricle (LV) also shows regression of hypertrophy (lower arrows in A). Ao, aorta; RV, right ventricle; LA, left atrium.
Figure 4 .

Evolution of the LVOTG after PTSMA. *p < 0.05; **p < 0.01; ***p < 0.0001 versus prior measurement.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Braunwald E. Induced septal infarction: a new therapeutic strategy for hypertrophic obstructive cardiomyopathy. Circulation. 1997 Apr 15;95(8):1981–1982. doi: 10.1161/01.cir.95.8.1981. [DOI] [PubMed] [Google Scholar]
- Brugada P., de Swart H., Smeets J. L., Wellens H. J. Transcoronary chemical ablation of ventricular tachycardia. Circulation. 1989 Mar;79(3):475–482. doi: 10.1161/01.cir.79.3.475. [DOI] [PubMed] [Google Scholar]
- Cleland J. G. The clinical course of heart failure and its modification by ACE inhibitors: insights from recent clinical trials. Eur Heart J. 1994 Jan;15(1):125–130. doi: 10.1093/oxfordjournals.eurheartj.a060364. [DOI] [PubMed] [Google Scholar]
- Faber L., Seggewiss H., Gleichmann U. Percutaneous transluminal septal myocardial ablation in hypertrophic obstructive cardiomyopathy: results with respect to intraprocedural myocardial contrast echocardiography. Circulation. 1998 Dec 1;98(22):2415–2421. doi: 10.1161/01.cir.98.22.2415. [DOI] [PubMed] [Google Scholar]
- Fananapazir L., Epstein N. D., Curiel R. V., Panza J. A., Tripodi D., McAreavey D. Long-term results of dual-chamber (DDD) pacing in obstructive hypertrophic cardiomyopathy. Evidence for progressive symptomatic and hemodynamic improvement and reduction of left ventricular hypertrophy. Circulation. 1994 Dec;90(6):2731–2742. doi: 10.1161/01.cir.90.6.2731. [DOI] [PubMed] [Google Scholar]
- Gleichmann U., Seggewiss H., Faber L., Fassbender D., Schmidt H. K., Strick S. Kathetertherapie der hypertrophen obstruktiven Kardiomyopathie. Dtsch Med Wochenschr. 1996 May 24;121(21):679–685. doi: 10.1055/s-2008-1043055. [DOI] [PubMed] [Google Scholar]
- Hina K., Kusachi S., Iwasaki K., Nogami K., Moritani H., Kita T., Taniguchi G., Tsuji T. Progression of left ventricular enlargement in patients with hypertrophic cardiomyopathy: incidence and prognostic value. Clin Cardiol. 1993 May;16(5):403–407. doi: 10.1002/clc.4960160507. [DOI] [PubMed] [Google Scholar]
- Kappenberger L., Linde C., Daubert C., McKenna W., Meisel E., Sadoul N., Chojnowska L., Guize L., Gras D., Jeanrenaud X. Pacing in hypertrophic obstructive cardiomyopathy. A randomized crossover study. PIC Study Group. Eur Heart J. 1997 Aug;18(8):1249–1256. doi: 10.1093/oxfordjournals.eurheartj.a015435. [DOI] [PubMed] [Google Scholar]
- Knight C., Kurbaan A. S., Seggewiss H., Henein M., Gunning M., Harrington D., Fassbender D., Gleichmann U., Sigwart U. Nonsurgical septal reduction for hypertrophic obstructive cardiomyopathy: outcome in the first series of patients. Circulation. 1997 Apr 15;95(8):2075–2081. doi: 10.1161/01.cir.95.8.2075. [DOI] [PubMed] [Google Scholar]
- Kuhn H., Gietzen F., Leuner C., Gerenkamp T. Induction of subaortic septal ischaemia to reduce obstruction in hypertrophic obstructive cardiomyopathy. Studies to develop a new catheter-based concept of treatment. Eur Heart J. 1997 May;18(5):846–851. doi: 10.1093/oxfordjournals.eurheartj.a015350. [DOI] [PubMed] [Google Scholar]
- MORROW A. G., BROCKENBROUGH E. C. Surgical treatment of idiopathic hypertrophic subaortic stenosis: technic and hemodynamic results of subaortic ventriculomyotomy. Ann Surg. 1961 Aug;154:181–189. doi: 10.1097/00000658-196108000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCully R. B., Nishimura R. A., Tajik A. J., Schaff H. V., Danielson G. K. Extent of clinical improvement after surgical treatment of hypertrophic obstructive cardiomyopathy. Circulation. 1996 Aug 1;94(3):467–471. doi: 10.1161/01.cir.94.3.467. [DOI] [PubMed] [Google Scholar]
- Nishimura R. A., Hayes D. L., Ilstrup D. M., Holmes D. R., Jr, Tajik A. J. Effect of dual-chamber pacing on systolic and diastolic function in patients with hypertrophic cardiomyopathy. Acute Doppler echocardiographic and catheterization hemodynamic study. J Am Coll Cardiol. 1996 Feb;27(2):421–430. doi: 10.1016/0735-1097(95)00445-9. [DOI] [PubMed] [Google Scholar]
- Pollick C., Rakowski H., Wigle E. D. Muscular subaortic stenosis: the quantitative relationship between systolic anterior motion and the pressure gradient. Circulation. 1984 Jan;69(1):43–49. doi: 10.1161/01.cir.69.1.43. [DOI] [PubMed] [Google Scholar]
- Sahn D. J., DeMaria A., Kisslo J., Weyman A. Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation. 1978 Dec;58(6):1072–1083. doi: 10.1161/01.cir.58.6.1072. [DOI] [PubMed] [Google Scholar]
- Seggewiss H., Gleichmann U., Faber L., Fassbender D., Schmidt H. K., Strick S. Percutaneous transluminal septal myocardial ablation in hypertrophic obstructive cardiomyopathy: acute results and 3-month follow-up in 25 patients. J Am Coll Cardiol. 1998 Feb;31(2):252–258. doi: 10.1016/s0735-1097(97)00508-1. [DOI] [PubMed] [Google Scholar]
- Sigwart U. Non-surgical myocardial reduction for hypertrophic obstructive cardiomyopathy. Lancet. 1995 Jul 22;346(8969):211–214. doi: 10.1016/s0140-6736(95)91267-3. [DOI] [PubMed] [Google Scholar]
- Spirito P., Seidman C. E., McKenna W. J., Maron B. J. The management of hypertrophic cardiomyopathy. N Engl J Med. 1997 Mar 13;336(11):775–785. doi: 10.1056/NEJM199703133361107. [DOI] [PubMed] [Google Scholar]
- Takagi E., Yamakado T., Nakano T. Prognosis of completely asymptomatic adult patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 1999 Jan;33(1):206–211. doi: 10.1016/s0735-1097(98)00555-5. [DOI] [PubMed] [Google Scholar]
- Wigle E. D., Rakowski H., Kimball B. P., Williams W. G. Hypertrophic cardiomyopathy. Clinical spectrum and treatment. Circulation. 1995 Oct 1;92(7):1680–1692. doi: 10.1161/01.cir.92.7.1680. [DOI] [PubMed] [Google Scholar]