

Abstract
OBJECTIVE—To report the initial and intermediate term results of stent implantation in children with coarctation of the aorta. PATIENTS AND DESIGN—17 patients with coarctation of the aorta underwent stent implantation (median age 11 years, range 0.4-15 years); six were treated for isolated coarctation, nine for recurrent coarctation (five after surgical repair and four after balloon dilatation), and two for complex long segment coarctation. INTERVENTIONS—The procedure was guided by a second catheter placed transseptally in the left ventricle or the aorta proximal to the coarctation site, for angiographic and haemodynamic monitoring during the procedure. Twenty two stents were implanted in 17 patients. One of the patients with long segment coarctation received four stents and the other three. Palmaz 4014 stents were placed in 11 patients, Palmaz 308 in five, and Palmaz 154 in one. RESULTS—Immediately after stent implantation the peak systolic gradient (mean (SD)) fell from 50.0 (24.5) to 2.1 (2.4) mm Hg (p < 0.05). The diameter of the stenotic lesion increased from 5.1 (1.5) mm to 13.9 (2.4) mm (p < 0.05). There were no deaths or procedure related complications. At a median follow up of 33 months, no cases of recoarctation were identified, either clinically (0/17; 0%, 95% confidence interval (CI) 0% to 19%) or angiographically (0/13; 0%, 95% CI 0% to 25%). CONCLUSIONS—Stent implantation for the treatment of coarctation of the aorta appears to have very low morbidity and mortality, and reasonable intermediate term results. Long term freedom from recoarctation using this method remains to be determined in comparison with simple balloon dilatation. Keywords: aortic coarctation; blood vessel prostheses; stents
Full Text
The Full Text of this article is available as a PDF (192.0 KB).
Figure 1 .
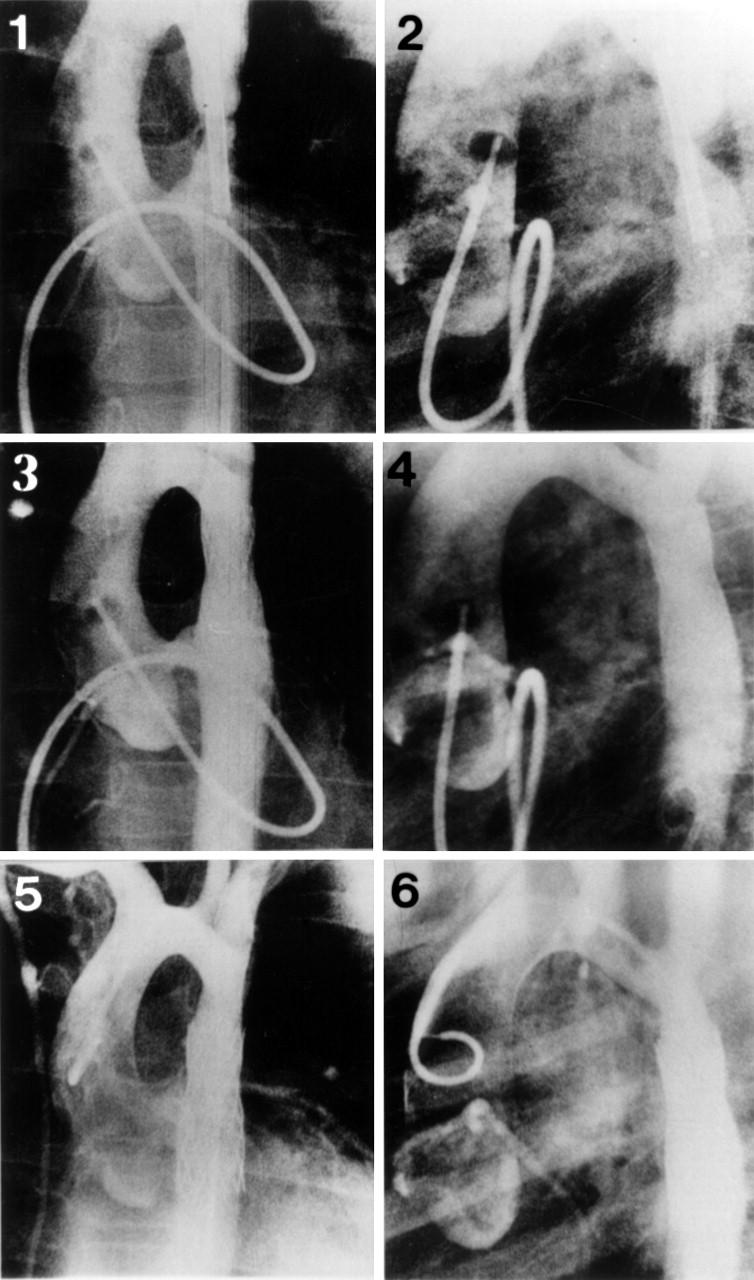
Antegrade ascending aortograms in the anteroposterior (1) and lateral (2) projections, showing the position of a stent across the coarctation before expansion. Repeat anteroposterior (3) and lateral (4) aortogram projections showed an aortic diameter of 13 mm at the stented segment and good stent position. Retrograde anteroposterior (5) and lateral (6) ascending aortogram projections 36 months later showed no evidence of restenosis and good stent position without fracture or displacement (patient 2, tables 1 and 2).
Figure 2 .

Antegrade ascending aortograms (left panels) and simultaneous ascending and descending aortic pressure tracings (right panels) obtained from a patient with long segment coarctation before (A) and immediately after (B) multiple stent implantation. An impressive increase in coarctation diameter and elimination of the pressure gradient across the coarctation is seen after deployment of the stents (patient 7, tables 1 and 2).
Figure 3 .
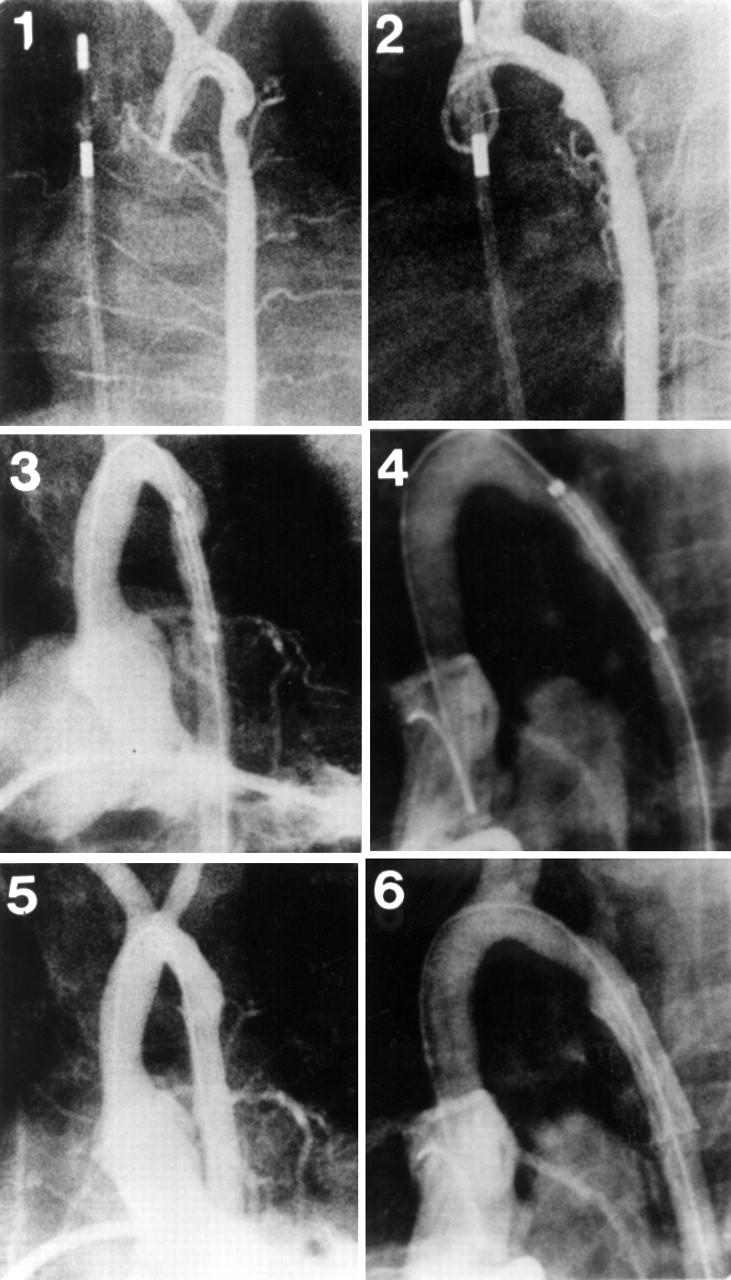
Ascending aortograms in the anteroposterior (1) and lateral (2) projections, revealing a discrete recoarctation in a 4 month old infant after a left subclavian flap operation. Left ventriculography in the anteroposterior (3) and lateral (4) projections show the position of a stent across the coarctation before expansion. Left ventriculography in the anteroposterior (5) and lateral (6) projections show a reasonable increase in coarctation diameter following stent placement (patient 1, tables 1 and 2).
Figure 4 .

Descending aortograms showing the treatment of a long segment coarctation of aorta with multiple stents. Picture 1 shows the upper part of the coarctation and picture 2 the lower part. Picture 3 shows the descending aorta immediately after placement of four stents. Pictures 4 and 5 show follow up aortograms one and six years after the procedure, respectively. There was no significant change in the aortic diameter at the stented area. Picture 6 shows a plain film radiograph six years after the procedure. Notice the mild stent dislodgement at the junctions between the first and second, as well as the third and fourth stents (arrowheads) (patient 7, tables 1 and 2).
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bulbul Z. R., Bruckheimer E., Love J. C., Fahey J. T., Hellenbrand W. E. Implantation of balloon-expandable stents for coarctation of the aorta: implantation data and short-term results. Cathet Cardiovasc Diagn. 1996 Sep;39(1):36–42. doi: 10.1002/(SICI)1097-0304(199609)39:1<36::AID-CCD7>3.0.CO;2-3. [DOI] [PubMed] [Google Scholar]
- Diethrich E. B., Heuser R. R., Cardenas J. R., Eckert J., Tarlian H. Endovascular techniques in adult aortic coarctation: the use of stents for native and recurrent coarctation repair. J Endovasc Surg. 1995 May;2(2):183–188. doi: 10.1583/1074-6218(1995)002<0183:ETIAAC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Ebeid M. R., Prieto L. R., Latson L. A. Use of balloon-expandable stents for coarctation of the aorta: initial results and intermediate-term follow-up. J Am Coll Cardiol. 1997 Dec;30(7):1847–1852. doi: 10.1016/s0735-1097(97)00408-7. [DOI] [PubMed] [Google Scholar]
- Fletcher S. E., Nihill M. R., Grifka R. G., O'Laughlin M. P., Mullins C. E. Balloon angioplasty of native coarctation of the aorta: midterm follow-up and prognostic factors. J Am Coll Cardiol. 1995 Mar 1;25(3):730–734. doi: 10.1016/0735-1097(94)00437-U. [DOI] [PubMed] [Google Scholar]
- Hakim F., Hawelleh A. A., Goussous Y., Hijazi Z. M. Simultaneous stent implantation for coarctation of the aorta and closure of patent ductus arteriosus using the Amplatzer duct occluder. Catheter Cardiovasc Interv. 1999 May;47(1):36–38. doi: 10.1002/(SICI)1522-726X(199905)47:1<36::AID-CCD6>3.0.CO;2-Q. [DOI] [PubMed] [Google Scholar]
- Hellenbrand W. E., Allen H. D., Golinko R. J., Hagler D. J., Lutin W., Kan J. Balloon angioplasty for aortic recoarctation: results of Valvuloplasty and Angioplasty of Congenital Anomalies Registry. Am J Cardiol. 1990 Mar 15;65(11):793–797. doi: 10.1016/0002-9149(90)91390-r. [DOI] [PubMed] [Google Scholar]
- Ing F. F., Goldberg B., Siegel D. H., Trachtman H., Bierman F. Z. Arterial stents in the management of neurofibromatosis and renovascular hypertension in a pediatric patient: case report of a new treatment modality. Cardiovasc Intervent Radiol. 1995 Nov-Dec;18(6):414–418. doi: 10.1007/BF00338313. [DOI] [PubMed] [Google Scholar]
- Ledesma M., Díaz y Díaz E., Alva Espinosa C., Sánchez Soberanes A., Martínez Sánchez A., Jiménez Arteaga S., Argüero R. Stents en coartación aórtica. Resultados inmediatos. Arch Inst Cardiol Mex. 1997 Sep-Oct;67(5):399–404. [PubMed] [Google Scholar]
- Mendelsohn A. M., Lloyd T. R., Crowley D. C., Sandhu S. K., Kocis K. C., Beekman R. H., 3rd Late follow-up of balloon angioplasty in children with a native coarctation of the aorta. Am J Cardiol. 1994 Oct 1;74(7):696–700. doi: 10.1016/0002-9149(94)90312-3. [DOI] [PubMed] [Google Scholar]
- O'Laughlin M. P., Perry S. B., Lock J. E., Mullins C. E. Use of endovascular stents in congenital heart disease. Circulation. 1991 Jun;83(6):1923–1939. doi: 10.1161/01.cir.83.6.1923. [DOI] [PubMed] [Google Scholar]
- Pedulla D. M., Grifka R. G., Mullins C. E., Allen D. Endovascular stent implantation for severe recoarctation of the aorta: case report with angiographic and 18-month clinical follow-up. Cathet Cardiovasc Diagn. 1997 Mar;40(3):311–314. doi: 10.1002/(sici)1097-0304(199703)40:3<311::aid-ccd22>3.0.co;2-q. [DOI] [PubMed] [Google Scholar]
- Rao P. S. Aortic rupture after balloon angioplasty of aortic coarctation. Am Heart J. 1993 Apr;125(4):1205–1206. doi: 10.1016/0002-8703(93)90150-8. [DOI] [PubMed] [Google Scholar]
- Redington A. N., Hayes A. M., Ho S. Y. Transcatheter stent implantation to treat aortic coarctation in infancy. Br Heart J. 1993 Jan;69(1):80–82. doi: 10.1136/hrt.69.1.80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Redington A. N., Weil J., Somerville J. Self expanding stents in congenital heart disease. Br Heart J. 1994 Oct;72(4):378–383. doi: 10.1136/hrt.72.4.378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg C., Weinstock D. J., Gold J. P., Notterman D. A. Measurements of central blood vessels in infants and children: normal values. Cathet Cardiovasc Diagn. 1992 Nov;27(3):197–201. doi: 10.1002/ccd.1810270308. [DOI] [PubMed] [Google Scholar]
- Suárez de Lezo J., Pan M., Romero M., Medina A., Segura J., Lafuente M., Pavlovic D., Hernández E., Melián F., Espada J. Immediate and follow-up findings after stent treatment for severe coarctation of aorta. Am J Cardiol. 1999 Feb 1;83(3):400–406. doi: 10.1016/s0002-9149(98)00877-7. [DOI] [PubMed] [Google Scholar]
- Suárez de Lezo J., Pan M., Romero M., Medina A., Segura J., Pavlovic D., Martinez C., Tejero I., Perez Navero J., Torres F. Balloon-expandable stent repair of severe coarctation of aorta. Am Heart J. 1995 May;129(5):1002–1008. doi: 10.1016/0002-8703(95)90123-x. [DOI] [PubMed] [Google Scholar]
- Thanopoulos B. V., Triposkiadis F., Margetakis A., Mullins C. E. Long segment coarctation of the thoracic aorta: treatment with multiple balloon-expandable stent implantation. Am Heart J. 1997 Apr;133(4):470–473. doi: 10.1016/s0002-8703(97)70194-7. [DOI] [PubMed] [Google Scholar]
- Tynan M., Finley J. P., Fontes V., Hess J., Kan J. Balloon angioplasty for the treatment of native coarctation: results of Valvuloplasty and Angioplasty of Congenital Anomalies Registry. Am J Cardiol. 1990 Mar 15;65(11):790–792. doi: 10.1016/0002-9149(90)91389-n. [DOI] [PubMed] [Google Scholar]