

Full Text
The Full Text of this article is available as a PDF (194.8 KB).
Figure 1: .

(A) Lesion created with radiofrequency energy one month previously in a canine ventricle. The lesion is pale, about 5 mm in diameter, and has smooth borders. (B) Histologic section of the same lesion. The lesion has a distinct border surrounded by normal myocardium, is hemispherical, and shows extensive fibrosis. The lesion depth is 6 mm.
Figure 2: .

(A) Schematic drawing of the two approaches which are available to ablate left sided accessory pathways. The retrograde aortic approach involves inserting the ablation catheter into the femoral artery and crossing the aortic valve to enter the left ventricle. The ablation catheter is positioned against the ventricular aspect of the mitral annulus. The transseptal approach involves crossing the interatrial septum and positioning a long transeptal sheath into the left atrium. The ablation catheter is then passed through the sheath and positioned against the atrial aspect of the mitral annulus at the site of the location of the accessory pathway. (B) The electrogram characteristics of a typical successful ablation site of an accessory pathway (ABL) are shown. Also shown are the surface leads I and V6 and intracardiac recordings obtained from the high right atrium (RA), the right ventricle apex (RV), the electrode catheter positioned to record a His bundle (HBE), and an electrode catheter positioned in the coronary sinus os (CS). The surface leads show a short PR interval and slurring of the upstroke of the QRS complex, which are characteristic of the pre-excitation pattern observed in patients with the Wolff-Parkinson-White syndrome. The interval from the His bundle recording (H) to onset of the QRS complex is less than 50 ms, confirming the presence of pre-excitation. At the successful ablation site, the ventricular electrogram (V) occurs very early relative to the onset of the QRS complex. Also observed is a discrete deflection between the atrial (A) and the ventricular components of the electrogram recorded at the ablation site, which is suggestive of an accessory pathway potential. (C) The disappearance of pre-excitation several seconds after onset of radiofrequency energy delivery during catheter ablation of an accessory pathway. Shown are the surface leads V1, I, V6, and the temperature recorded from the ablation catheter. The temperature recorded from the ablation electrode increases from 37°C to 66°C within two seconds of radiofrequency energy delivery. Pre-excitation resolves several seconds thereafter.
Figure 3: .
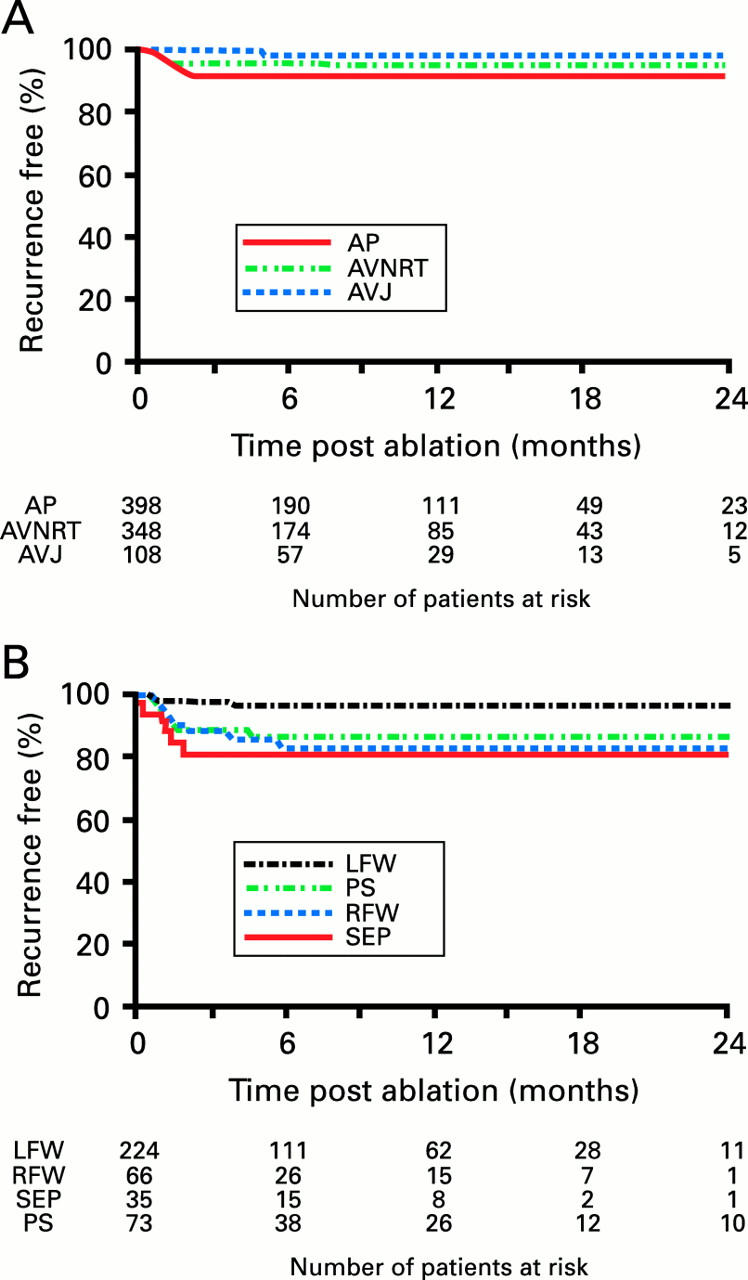
(A) Kaplan-Meier curve showing freedom from arrhythmia recurrence among patients who underwent successful ablation of an accessory pathway (AP), atrioventricular nodal re-entrant tachycardia (AVNRT), or atrioventricular junction (AVJ). (B) Kaplan-Meier curve showing freedom from arrhythmia recurrence among patients who underwent successful ablation of an accessory pathway subclassified by its location. LFW, left free wall; RFW, right free wall; PS, posteroseptal; SEP, septal. Reproduced from Calkins et al, Circulation 1999;99:262-70, with permission of the publisher.
Figure 4: .
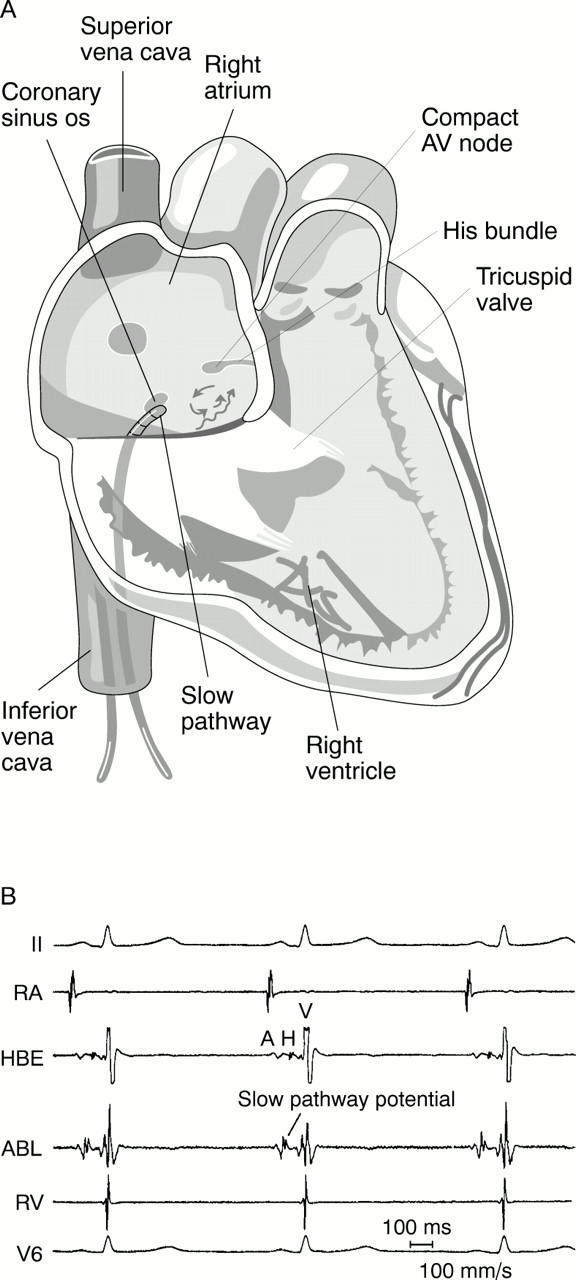
(A) Schematic drawing of the posterior or "slow pathway" approach to catheter ablation of atrioventricular nodal re-entrant tachycardia (AVNRT). The ablation catheter is positioned anterior to the coronary sinus os. A schematic drawing of the hypothesised re-entrant circuit for AVNRT is also shown. (B) The electrogram of a successful slow pathway ablation site. Also shown are surface leads 1 and V6 and intracardiac recordings obtained from the right atrium, the right ventricle, and the electrode catheter positioned to record a His bundle. The intracardiac electrogram at the ablation site reveals a ventricular electrogram substantially larger than the atrial electrogram, and a distinct deflection consistent with a slow pathway potential immediately after the atrial electrogram. The arrow points to a slow pathway potential.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Baker B. M., Lindsay B. D., Bromberg B. I., Frazier D. W., Cain M. E., Smith J. M. Catheter ablation of clinical intraatrial reentrant tachycardias resulting from previous atrial surgery: localizing and transecting the critical isthmus. J Am Coll Cardiol. 1996 Aug;28(2):411–417. doi: 10.1016/0735-1097(96)00154-4. [DOI] [PubMed] [Google Scholar]
- Calkins H., Kim Y. N., Schmaltz S., Sousa J., el-Atassi R., Leon A., Kadish A., Langberg J. J., Morady F. Electrogram criteria for identification of appropriate target sites for radiofrequency catheter ablation of accessory atrioventricular connections. Circulation. 1992 Feb;85(2):565–573. doi: 10.1161/01.cir.85.2.565. [DOI] [PubMed] [Google Scholar]
- Calkins H., Prystowsky E., Berger R. D., Saul J. P., Klein L. S., Liem L. B., Huang S. K., Gillette P., Yong P., Carlson M. Recurrence of conduction following radiofrequency catheter ablation procedures: relationship to ablation target and electrode temperature. The Atakr Multicenter Investigators Group. J Cardiovasc Electrophysiol. 1996 Aug;7(8):704–712. doi: 10.1111/j.1540-8167.1996.tb00578.x. [DOI] [PubMed] [Google Scholar]
- Calkins H., Sousa J., el-Atassi R., Rosenheck S., de Buitleir M., Kou W. H., Kadish A. H., Langberg J. J., Morady F. Diagnosis and cure of the Wolff-Parkinson-White syndrome or paroxysmal supraventricular tachycardias during a single electrophysiologic test. N Engl J Med. 1991 Jun 6;324(23):1612–1618. doi: 10.1056/NEJM199106063242302. [DOI] [PubMed] [Google Scholar]
- Calkins H., Yong P., Miller J. M., Olshansky B., Carlson M., Saul J. P., Huang S. K., Liem L. B., Klein L. S., Moser S. A. Catheter ablation of accessory pathways, atrioventricular nodal reentrant tachycardia, and the atrioventricular junction: final results of a prospective, multicenter clinical trial. The Atakr Multicenter Investigators Group. Circulation. 1999 Jan 19;99(2):262–270. doi: 10.1161/01.cir.99.2.262. [DOI] [PubMed] [Google Scholar]
- Calkins H., Yong P., Miller J. M., Olshansky B., Carlson M., Saul J. P., Huang S. K., Liem L. B., Klein L. S., Moser S. A. Catheter ablation of accessory pathways, atrioventricular nodal reentrant tachycardia, and the atrioventricular junction: final results of a prospective, multicenter clinical trial. The Atakr Multicenter Investigators Group. Circulation. 1999 Jan 19;99(2):262–270. doi: 10.1161/01.cir.99.2.262. [DOI] [PubMed] [Google Scholar]
- Chen S. A., Chiang C. E., Yang C. J., Cheng C. C., Wu T. J., Wang S. P., Chiang B. N., Chang M. S. Sustained atrial tachycardia in adult patients. Electrophysiological characteristics, pharmacological response, possible mechanisms, and effects of radiofrequency ablation. Circulation. 1994 Sep;90(3):1262–1278. doi: 10.1161/01.cir.90.3.1262. [DOI] [PubMed] [Google Scholar]
- Chen S. A., Tai C. T., Chiang C. E., Ding Y. A., Chang M. S. Focal atrial tachycardia: reanalysis of the clinical and electrophysiologic characteristics and prediction of successful radiofrequency ablation. J Cardiovasc Electrophysiol. 1998 Apr;9(4):355–365. doi: 10.1111/j.1540-8167.1998.tb00924.x. [DOI] [PubMed] [Google Scholar]
- Curtis A. B., Kutalek S. P., Prior M., Newhouse T. T. Prevalence and characteristics of escape rhythms after radiofrequency ablation of the atrioventricular junction: results from the registry for AV junction ablation and pacing in atrial fibrillation. Ablate and Pace Trial Investigators. Am Heart J. 2000 Jan;139(1 Pt 1):122–125. doi: 10.1016/s0002-8703(00)90318-1. [DOI] [PubMed] [Google Scholar]
- Dinerman J. L., Berger R. D., Calkins H. Temperature monitoring during radiofrequency ablation. J Cardiovasc Electrophysiol. 1996 Feb;7(2):163–173. doi: 10.1111/j.1540-8167.1996.tb00511.x. [DOI] [PubMed] [Google Scholar]
- Haissaguerre M., Gaita F., Fischer B., Commenges D., Montserrat P., d'Ivernois C., Lemetayer P., Warin J. F. Elimination of atrioventricular nodal reentrant tachycardia using discrete slow potentials to guide application of radiofrequency energy. Circulation. 1992 Jun;85(6):2162–2175. doi: 10.1161/01.cir.85.6.2162. [DOI] [PubMed] [Google Scholar]
- Jackman W. M., Beckman K. J., McClelland J. H., Wang X., Friday K. J., Roman C. A., Moulton K. P., Twidale N., Hazlitt H. A., Prior M. I. Treatment of supraventricular tachycardia due to atrioventricular nodal reentry, by radiofrequency catheter ablation of slow-pathway conduction. N Engl J Med. 1992 Jul 30;327(5):313–318. doi: 10.1056/NEJM199207303270504. [DOI] [PubMed] [Google Scholar]
- Jackman W. M., Wang X. Z., Friday K. J., Roman C. A., Moulton K. P., Beckman K. J., McClelland J. H., Twidale N., Hazlitt H. A., Prior M. I. Catheter ablation of accessory atrioventricular pathways (Wolff-Parkinson-White syndrome) by radiofrequency current. N Engl J Med. 1991 Jun 6;324(23):1605–1611. doi: 10.1056/NEJM199106063242301. [DOI] [PubMed] [Google Scholar]
- Kalbfleisch S. J., el-Atassi R., Calkins H., Langberg J. J., Morady F. Safety, feasibility and cost of outpatient radiofrequency catheter ablation of accessory atrioventricular connections. J Am Coll Cardiol. 1993 Mar 1;21(3):567–570. doi: 10.1016/0735-1097(93)90086-g. [DOI] [PubMed] [Google Scholar]
- Lee R. J., Kalman J. M., Fitzpatrick A. P., Epstein L. M., Fisher W. G., Olgin J. E., Lesh M. D., Scheinman M. M. Radiofrequency catheter modification of the sinus node for "inappropriate" sinus tachycardia. Circulation. 1995 Nov 15;92(10):2919–2928. doi: 10.1161/01.cir.92.10.2919. [DOI] [PubMed] [Google Scholar]
- Lesh M. D., Kalman J. M., Saxon L. A., Dorostkar P. C. Electrophysiology of "incisional" reentrant atrial tachycardia complicating surgery for congenital heart disease. Pacing Clin Electrophysiol. 1997 Aug;20(8 Pt 2):2107–2111. doi: 10.1111/j.1540-8159.1997.tb03638.x. [DOI] [PubMed] [Google Scholar]
- Lesh M. D., Van Hare G. F., Scheinman M. M., Ports T. A., Epstein L. A. Comparison of the retrograde and transseptal methods for ablation of left free wall accessory pathways. J Am Coll Cardiol. 1993 Aug;22(2):542–549. doi: 10.1016/0735-1097(93)90062-6. [DOI] [PubMed] [Google Scholar]
- Low P. A., Opfer-Gehrking T. L., Textor S. C., Benarroch E. E., Shen W. K., Schondorf R., Suarez G. A., Rummans T. A. Postural tachycardia syndrome (POTS). Neurology. 1995 Apr;45(4 Suppl 5):S19–S25. [PubMed] [Google Scholar]
- Scheinman M. M., Huang S. The 1998 NASPE prospective catheter ablation registry. Pacing Clin Electrophysiol. 2000 Jun;23(6):1020–1028. doi: 10.1111/j.1540-8159.2000.tb00891.x. [DOI] [PubMed] [Google Scholar]
- Sousa J., el-Atassi R., Rosenheck S., Calkins H., Langberg J., Morady F. Radiofrequency catheter ablation of the atrioventricular junction from the left ventricle. Circulation. 1991 Aug;84(2):567–571. doi: 10.1161/01.cir.84.2.567. [DOI] [PubMed] [Google Scholar]
- de Buitleir M., Sousa J., Bolling S. F., el-Atassi R., Calkins H., Langberg J. J., Kou W. H., Morady F. Reduction in medical care cost associated with radiofrequency catheter ablation of accessory pathways. Am J Cardiol. 1991 Dec 15;68(17):1656–1661. doi: 10.1016/0002-9149(91)90325-f. [DOI] [PubMed] [Google Scholar]