

Abstract
A 5 month old girl had typical clinical features of acute myocarditis just after the febrile period of exanthem subitum and died immediately. She had been healthy, with normal development, and there was no family history of particular note. Myocardial postmortem findings were compatible with acute myocarditis. Although the isolation of human herpesvirus 6 (HHV-6) was not attempted, positive IgM antibody to HHV-6 was detected in the patient's serum. Moreover, HHV-6 variant B DNA was detected in several tissues, including myocardium, by the polymerase chain reaction (PCR). In contrast, antibody responses to human herpesvirus 7, another causal agent of exanthem subitum, were not found, and enteroviral RNA was not detected in myocardial tissues by reverse transcription PCR. Apoptotic changes were seen in infiltrating cells within the myocardial tissues by means of the TUNEL method. HHV-6 antigen was not detected in several tissues (including myocardium) by immunohistochemical analysis. In conclusion, HHV-6 may have been the causative agent of fatal acute myocarditis in this infant.
Key Words: human herpesvirus 6 • myocarditis • polymerase chain reaction
Full Text
The Full Text of this article is available as a PDF (179.6 KB).

Figure 1 Diffuse infiltration of mononuclear cells and neutrophils is seen in the myocardium with oedematous change and degeneration and loss of myocardial cells (haematoxylin and eosin stained; original magnification, x200).

Figure 2 Infiltrating mononuclear cells in the myocardium are confirmed to be apoptotic by means of the TUNEL method using an ApoTag peroxidase kit (DAB-peroxidase; original magnification, x200).
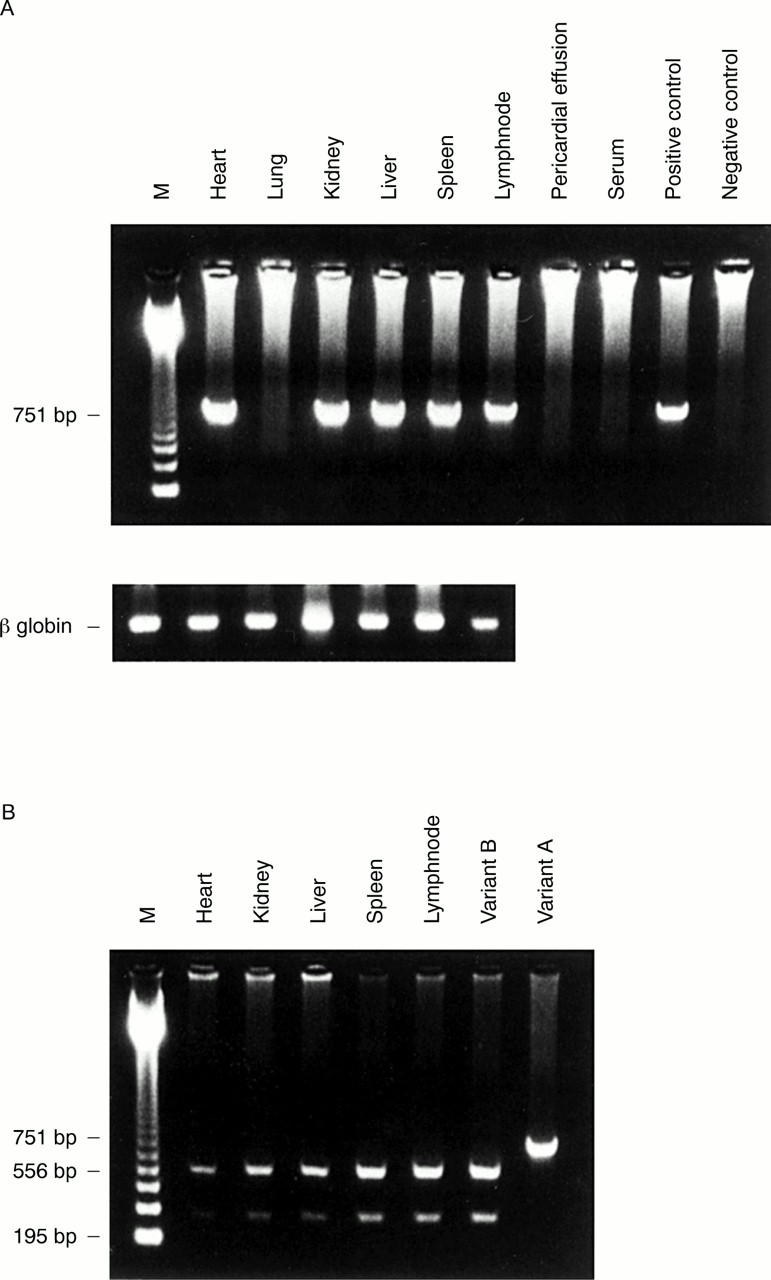
Figure 3 (A) Human herpesvirus 6 (HHV-6) DNA amplified by nested PCR. Positive bands are seen in the lanes indicating heart, liver, kidney, spleen, and lymph node. The ß globin gene was amplified in all DNA specimens. (B) Second round PCR products extracted from heart, kidney, liver, spleen, and lymph node were digested in an HHV-6 variant B specific manner by HindIII. Variant B, FG-1 strain isolated from a patient with exanthem subitum in our facility; variant A, GS strain.