

Abstract
Background: Mean-body temperature (MBT) is the mass-weighted average temperature of body tissues. Core temperature is easy to measure, but direct measurement of peripheral tissue temperature is painful, risky, and requires complex calculations. Alternatively MBT can be estimated from core and mean skin temperatures with a formula proposed by Burton in 1935: MBT = 0.64. TCore + 0.36. TSkin. This formula remains widely used, but not been validated in the perioperative period and seems unlikely to remain accurate in dynamic perioperative conditions such as cardiopulmonary bypass. We thus tested the hypothesis that MBT, as estimated with Burton’s formula, poorly estimates measured MBT at a temperature range between 18 and 36.5° C.
Materials and Methods: We re-evaluated four of our previously published studies in which core and mass-weighted mean peripheral tissue temperatures were measured in patients undergoing substantial thermal perturbations. Peripheral compartment temperatures were estimated using fourth-order regression and integration over volume from 18 intramuscular needle thermocouples, 9 skin temperatures, and "deep" hand and foot temperature. MBT was determined from mass-weighted average of core and peripheral tissue temperatures and estimated from core temperature and mean skin temperature (15 area-weighted sites) using Burton’s formula.
Results: 913 data pairs from 44 study subjects were included in the analysis. Measured MBT ranged from 18 to 36.5°C. There was a remarkably good relationship between measured and estimated MBT: MBTmeasured = 0.94 · MBTestimated + 2.15, r2 = 0.98. Differences between the estimated and measured values averaged -0.09 ± 0.42°C.
Conclusions: We concluded that estimation of MBT from mean skin and core temperatures is generally accurate and precise.
Introduction
Since the specific heat of human tissue is relatively well established, body heat content can be calculated from mean-body temperature (MBT). Mean-body temperature, defined as the mass-weighted average of tissue temperatures throughout the body, is thus a fundamental characterization of a person’s thermal status. Body heat distribution can be modeled as two thermal compartments, namely the core (trunk and head) and peripheral tissues (the extremities).
Even in a moderate environment, average temperature of the peripheral thermal compartment is 2-4°C less than core temperature.1 However, this thermal gradient can range from nearly zero to large values depending on the severity of the environment and the consequent vasomotor responses. The perioperative period is dynamic and associated with substantial changes in the core-to-peripheral tissue temperature gradient and internal distribution of body heat. For example, induction of general anesthesia is associated with a substantial flow of heat from the core to peripheral tissues because anesthetics reduce the vasoconstriction threshold (triggering core temperature) by 2 to 4°C.2 Vasoconstriction then recurs in patients who become sufficiently hypothermic, usually at a core temperature of approximately 34.5°C; this vasoconstriction constrains metabolic heat to the core thermal compartment and eventually restores the normal core-to-peripheral thermal gradient.3 Because vasomotion has such an important effect on the distribution of body heat in the perioperative period, it would be difficult to predict mean-body temperature from core temperature alone.
Core temperature is easy to measure and temperatures are relatively homogeneous throughout the trunk and head; it is thus easy to determine average temperature of the core thermal compartment. Peripheral tissue temperatures, on the other hand, vary widely depending on the region, environmental characteristics, and thermoregulatory vasomotion. Direct measurement of peripheral tissue temperature is difficult, but can be accomplished by insertion of a sufficient number of needle thermocouples, combined with tedious calculations. This procedure is complex, painful, and risky.
In 1935 Burton4 cleverly proposed that mean-body temperature could be calculated from a formula: MBT = a. TCore + (1-a). TSkin. The general form of the equation was based on the logic that core tissues are relatively homogeneous whereas tissue temperature in the peripheral decreases parabolically from core temperature to skin temperature. The value of a, the coefficient describing the contribution of core temperature to mean-body temperature, was then estimated by simultaneously measuring the change in body heat content (in a calorimeter), core temperature, and mean-skin temperature. The resulting value of the coefficient alpha was 0.64, thus giving the formula: MBT = 0.64. TCore + 0.36. TSkin.
A similar approach has been used by others, including Hardy and DuBois,5 who proposed a coefficient, a, of 0.7 for a neutral environment; Stolwijk and Hardy,6 who proposed a coefficient of 0.7 for a hot environment; and Snellen,7 who found the coefficient to be ≈0.8 during muscular work in a hot environment. Subsequently, Colin et al.8 showed in an elegant study that Burton’s coefficient was correct for a neutral environment, but that the coefficient increased to 0.79 in an extremely warm environment.
Surely the most severe thermal stress humans endure is hypothermic cardiopulmonary bypass. Bypass machines, through which the entire circulation flows, contains powerful heat exchangers that can essentially set blood temperature to any desired value. Consequently, it is quite possible — and hardly unusual — to change core temperature at rates approaching a degree centigrade per minute. The changes are especially notable when patients are cooled to core temperatures near 18°C for circulatory arrest during repairs of complex cardiac, aortic arch, and brain abnormalities.9 In these patients especially, it would be virtually impossible to predict mean-body temperature from core temperature alone, especially during periods of rapid thermal perturbation.
It is similarly by no means obvious that a simple combination of mean-skin and core temperatures will accurately reflect average temperature of human tissues under such dynamic perioperative conditions. Certainly Burton’s formula4 and its successor8 were not designed for, nor validated under, such circumstances. We thus tested Burton’s approach in the perioperative period because a formula that remains valid in the face of such large tissue-temperature inhomogeneities and rapid flows of heat from the core to the periphery is likely to be generally applicable.
Materials and Methods
We evaluated four previously published heat balance studies; in each, patients underwent substantial thermal perturbations. Two studies evaluated core and peripheral temperatures in patients undergoing cardiac surgery during extracorporeal circulation9,10; one evaluated heat balance during anesthesia and induced fever11; and the fourth tested the efficacy of an endovascular heat-exchanging catheter in healthy human volunteers.12 In each case, mean-body temperature was calculated and estimated at 15-minute intervals.
Arm and leg tissue temperatures were determined as previously described.13 In each subject, the leg was divided into five segments: upper thigh, lower thigh, upper calf, lower calf, and foot. Each thigh and calf segment was further divided into an anterior and posterior section, with one third of the estimated mass considered to be posterior. At each circumference, leg muscle temperatures were recorded using 8-, 18-, and 38-mm-long, 21-g, needle thermocouples (Tyco-Mallinckrodt Anesthesiology Products, Inc.) inserted perpendicular to the skin surface. Skin-surface temperatures were recorded immediately adjacent to each set of needles and directly posterior to each set. Subcutaneous temperature was measured on the ball of the foot and palm using deep-tissue thermometers (Terumo Medical Corp., Tokyo, Japan).14,15 These devices estimate tissue temperature ≈1 cm below the skin surface.
Anterior segment tissue temperatures, as a function of radial distance from the center of the leg segment, were calculated using skin-surface and muscle temperatures and fourth-order regressions. Temperature at the center of the thigh was assumed to equal core temperature. In contrast, temperature at the center of the lower leg segments was estimated from the regression equation with no similar assumption. Average anterior limb temperature was estimated from these individual temperatures using the fourth-order version of a previously described formula 13: (Equation 1) where TAve is average temperature of the leg segment from the center to radius r and a2 (°C/cm2) and a4 (°C/cm4) are the fourth-order regression constants.
Rather than assume full radial symmetry, we assumed only that radial temperature distribution in the posterior leg segments would also be parabolic. Accordingly, we calculated the regression constant a2 in the posterior leg segments from a0 determined from the adjacent anterior segment and the posterior segment skin temperature. Average posterior segment tissue temperatures were then determined from the second-order version of Equation 1. We have previously described the derivation of these equations and their limitations.13
"Deep temperature," measured on the ball of the foot, was assumed to represent the entire foot. Average temperatures of the thigh and lower leg (calf and foot) were calculated by weighting values from each of the nine segments in proportion to their estimated masses. The right and left legs were treated comparably throughout this study, so we assumed that average tissue temperatures in the two limbs were similar.
The lengths of the right arm (axilla to elbow) and forearm (elbow to wrist) were measured in cm. The circumference was measured at the mid-point of each segment. As in the right leg, 8-, 18-, and 38-mm-long needle thermocouples were inserted into each segment. Skin-surface temperatures were recorded immediately adjacent to each set of needles.
Average arm tissue temperatures were calculated from parabolic tissue temperature regressions and the equation above. In the arms, we assumed full radial symmetry and thus did not separately calculate posterior segment values. Adductor pollicis temperature was assumed to represent that of the entire hand. As in the leg, average temperatures of the arm and forearm (forearm and hand) were calculated by weighting values from each of the three segments in proportion to their estimated masses.
Trunk and head weight was estimated by subtracting the calculated weight of the extremities (from the radial integration) from the total weight of each subject. Measured mean-body temperature was determined from the mass-weighted average of core and peripheral tissue temperatures.
Area-weighted, mean skin-surface temperature was computed from measurements at 15 sites by assigning the following regional percentages to each area: head—6%, upper arms—9%, forearms—6%, hands—2.5%, fingers—2%, back—19%, chest—9.5%, abdomen—9.5%, medial thigh—6%, lateral thigh—6% posterior thigh—7%, anterior calves—7.5%, posterior calves— 4%, feet—4%, and toes—2%.16 Mean-body temperature was estimated from mean-skin and core temperatures using the formula of Burton4 MBT = 0.64. TCore + 0.36. TSkin. Measured and estimated MBTs were compared using linear regression and Bland-Altman analysis.17 Results are presented as means ± SDs (95% confidence intervals).
Results
We included 913 data pairs from four studies in the analysis (44 study subjects) (11, 14-16). Morphometric and demographic characteristics, and study details are presented in Table 1. Core temperature ranged from 18.5 to 37.1°C and measured MBT ranged from 18 to 36.5°C. There was a remarkably good relationship between measured and estimated MBT: MBTmeasured = 0.94 · MBTestimated + 2.15, r2 = 0.98 (Fig. 1).
The bias (average difference between estimated and measured mean-body temperature) was -0.09 ± 0.42°C, solid line on Fig 2, (95% confidence interval -0.12 to -0.06°C). The precision (average of the absolute value of the difference between estimated and measured mean-body temperature) was 0.31 ± 0.29, (95% confidence interval -0.29 to 0.33°C). Over the entire dataset, 87% of the mean-body temperature estimates were within 0.5°C of the measured values and 92% were within 0.7°C.
Differences between estimated and measured values were greatest during deep hypothermia (mean-body temperature < 31°C for cardiopulmonary bypass)9 and during pyrogen-induced fever.11 When the analysis was restricted to the remaining two studies,10,12 the bias (average difference between estimated and measured mean-body temperature) was - 0.15 ± 0.33°C, solid line on Fig 3, (95% confidence interval -0.18 to -0.12°C). The precision (average of the absolute value of the difference between estimated and measured mean-body temperature) was 0.28 ± 0.23, (95% confidence interval -0.26 to 0.30°C). Over the entire dataset, 91% of the mean-body temperature estimates were within 0.5°C of the measured values.
Discussion
To our surprise, Burton’s formula worked remarkably well over the entire tested range of mean-body temperatures from 31°C to 36.5°C. Even over this enormous range, the average difference between estimated and measured mean-body temperatures was -0.09 ± 0.42°C. As might be expected, the formula was somewhat less accurate at the coldest temperatures, and especially poor during the rapid cooling phase. This is because only a relatively small volume of the core was initially cooled, but the Burton formula assumes that 64% of the body mass is represented by core temperature — a fraction that is obviously not the case during rapid cooling. For less obvious reasons, the formula was also less accurate during fever in several volunteers, but not in all of them.
Nonetheless, our results suggest that Burton’s formula is generally accurate over a wide range of circumstances and can be substituted for direct measurements that are invasive and painful. It is important to recognize, however, that an error of 0.5°C in mean-body temperature corresponds to 29 kcal in a 70-kg person. Hence, Burton’s formula should be used cautiously in applications where accurate detection of small changes in body heat content is required. Fortunately, previous work4,8 indicates that the formula is highly accurate in near steady-state neutral conditions.
A limitation of our study is that our determination of average peripheral tissue temperature is imperfect because it is based on a limited number of measurements and a number of approximations. For example, our calculation of leg heat content assumes radial symmetry. To minimize risk to our volunteers, we did not verify this assumption by inserting more than three needles in each leg segment. It remains likely that tissue heat content in the posterior third of the leg decreased somewhat less than estimated because heat loss from this region was minimized by the foam insulation covering the operating table. Nonetheless, given the cylindrical shape of the leg and the central position of its major blood vessels, tissue temperatures are likely to be roughly symmetrical. An assumption of angular symmetry is used in nearly all models of heat balance, including some that have been extensively validated.18
Our calculations make the further assumption that each leg segment is cylindrical. Although not strictly accurate, a cylinder is a reasonable approximation of leg shape and simplifies analysis. Once again, most heat balance models make this assumption and still produce experimentally verifiable results.18 Finally, hand and foot temperature was estimated from "deep temperatures." Deep temperatures are at best an approximation of average tissue temperature in these inhomogeneous structures; fortunately, both the hands and feet are small and thus contribute relatively little to mean-body temperature. Despite the limitations of our tissue temperature measurements, changes in body heat content determined from these measurements are similar to those determined from metabolic rate and cutaneous heat loss.19 These data suggest that the tissue measurements are not far wrong.
Rectal temperature often differs substantially from true core-body temperature, especially during rapid thermal transients.20-22 Given this limitation, rectal temperature appears to be sub-optimal even for routine clinical use, to say nothing of thermoregulatory research. We thus measured core-body temperature at the tympanic membrane,11 nasopharynx,9,10 or distal esophagus12 in our studies. Each was appropriate for the circumstances of the studies. For example, distal esophageal temperature is usually the best minimally invasive core temperature measurement site, but is subject to artifact during cardiopulmonary bypass and accordingly less reliable than the nasopharynx in these patients. Tympanic membrane temperatures are accurate so long as the thermocouple is properly position, the ear canal is occluded, and the face is protected from direct thermal manipulation — as was the case here.
In summary, direct measurement of peripheral tissue temperature can be accomplished by insertion of sufficient needle thermocouples, combined with relatively complex calculations; the procedure is complex, painful, and risky. An alternative is a simple formula, based on core and mean-skin temperatures, proposed by Burton. However, this formula has not been well validated. We thus compared the two methods and found, perhaps surprisingly, that Burton’s formula worked well — even during severe thermal perturbations — over the range of core temperatures from 18.5 to 37.1°C. The formula was especially accurate when core temperatures were between 31 and 36.5°C, with the estimated temperatures differing from measured values by only - 0.09 ± 0.42°C. We conclude that Burton’s 1935 formula is remarkably accurate and precise.
Fig. 1.

Linear regression including all 913 data pairs from 44 subjects.9-12 Mean-body temperature (MBT) was estimated from core (Tcore) and mean-skin (TSkin) temperature and compared to directly measured values. There was a remarkably good relationship between measured and estimated mean-body temperatures: .
Fig. 2.
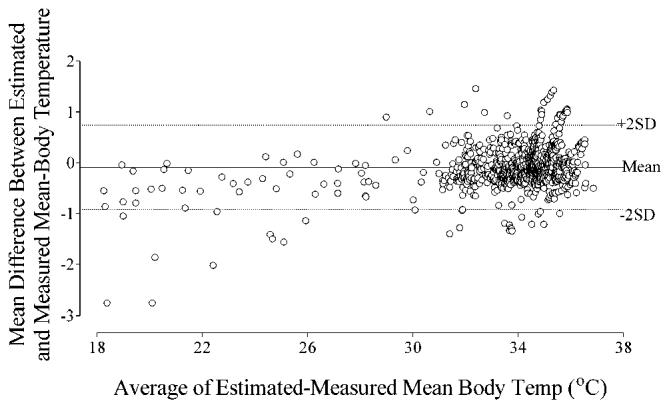
Bland-Altman plot for all 913 data pairs from all four studies.9-12 The bias (average difference between estimated and measured mean-body temperature) is - 0.09 ± 0.42°C, solid line on figure, (95% confidence interval -0.12 to -0.06°C). The precision (average of the absolute value of the difference between estimated and measured mean-body temperature) is 0.31 ± 0.29, (95% confidence interval -0.29 to 0.33°C). Over the entire dataset, 87% of the mean-body temperature estimates were within 0.5°C of the measured values.
Fig. 3.
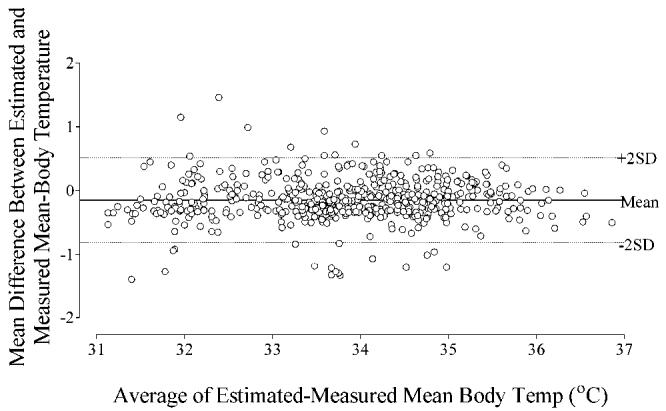
Bland-Altman plot of 535 data pairs10,12 when the studies of deep hypothermia for circulatory arrest9 and fever11 were excluded. The bias (average difference between estimated and measured mean-body temperature) is -0.15 ± 0.33°C, solid line on figure, (95% confidence interval -0.18 to -0.12°C). The precision (average of the absolute value of the difference between estimated and measured mean-body temperature) is 0.28 ± 0.23, (95% confidence interval -0.26 to 0.30°C). Over the entire dataset, 91% of the mean-body temperature estimates were within 0.5°C of the measured values.
Table 1.
Morphometric and Demographic Characteristics, and Study Details.
| Bypass at 17°C | Bypass at 32°C | Fever | Endovascular Heat Exchanger | |
|---|---|---|---|---|
| Age (yr) | 59 ± 11 | 62 ± 12 | 28 ± 3 | 22 ± 3 |
| Weight (kg) | 84 ± 17 | 78 ± 10 | 78 ± 9 | 67 ± 9 |
| Sex (M / F) | 5/3 | 16/4 | 7/0 | 6/3 |
| Height (cm) | 172 ± 7 | 171 ± 7 | 174 ± 5 | 175 ± 8 |
| Subjects | Cardiac Patients | Cardiac Patients | Healthy Volunteers | Healthy Volunteers |
| Core Temperature Measurement Site (°C) | Nasopharynx | Nasopharynx | Tympanic Membrane | Distal Esophagus |
| Maximum Core Temperature (°C) | 36.5 ± 0.3 | 36.8 ± 0.4 | 37.6 ± 0.9 | 37.6 ± 0.9 |
| Minimum Core Temperature (°C) | 16.8 ± 1.1 | 31.7 ± 0.5 | 36.5 ± 0.3 | 36.5 ± 0.3 |
| Paired Measurements (number) | 95 | 288 | 292 | 238 |
We evaluated estimated and measured mean-body temperature in subjects who participated in four studies. Two studies evaluated core and peripheral temperatures in patients undergoing cardiac surgery during extracorporeal circulation9,10; one evaluated heat balance during anesthesia and induced fever 11; and the fourth tested the efficacy of an endovascular heat-exchanging catheter in healthy human volunteers.12
Footnotes
Supported by NIH Grant GM 061655 (Bethesda, MD), the Gheens Foundation (Louisville, KY), the Joseph Drown Foundation (Los Angeles, CA), and the Commonwealth of Kentucky Research Challenge Trust Fund (Louisville, KY). Mallinckrodt Anesthesiology Products, Inc. (St. Louis, MO) donated the thermocouples we used. We thank Gilbert Haugh, M.S., for the statistical analysis and Nancy Alsip, Ph.D., for editorial assistance (both from the OUTCOMES RESEARCH Institute at the University of Louisville).
References
- 1.Rajek A, Greif R, Sessler DI, Baumgardner J, Laciny S, Bastanmehr H. Core cooling by central-venous infusion of 4°C and 20°C fluid: Isolation of core and peripheral thermal compartments. Anesthesiology. 2000;93:629–637. doi: 10.1097/00000542-200009000-00010. [DOI] [PubMed] [Google Scholar]
- 2.Xiong J, Kurz A, Sessler DI, Plattner O, Christensen R, Dechert M, Ikeda T. Isoflurane produces marked and non-linear decreases in the vasoconstriction and shivering thresholds. Anesthesiology. 1996;85:240–245. doi: 10.1097/00000542-199608000-00003. [DOI] [PubMed] [Google Scholar]
- 3.Kurz A, Sessler DI, Christensen R, Dechert M. Heat balance and distribution during the core-temperature plateau in anesthetized humans. Anesthesiology. 1995;83:491–499. doi: 10.1097/00000542-199509000-00007. [DOI] [PubMed] [Google Scholar]
- 4.Burton AC. Human Calorimetry: The average temperature of the tissues of the body. J Nutr. 1935;9:261–280. [Google Scholar]
- 5.Hardy JD, DuBois EF. Basal metabolism, radiation, convection, and evaporation at temperatre from 22° to 35° C. J Nutr. 1938;15:477–492. [Google Scholar]
- 6.Stolwijk JAJ, Hardy JD. Partitional calorimetric studies of responses of man to thermal transients. J Appl Physiol. 1966;21:967–977. doi: 10.1152/jappl.1966.21.3.967. [DOI] [PubMed] [Google Scholar]
- 7.Snellen JW. Mean body temperaure and the control of sweating. Acta Physiol Neerl. 1966;14:99–174. [PubMed] [Google Scholar]
- 8.Colin J, Timbal J, Houdas Y, Boutelier C, Guieu JD. Computation of mean body temperature from rectal and skin temperatures. J Appl Physiol. 1971;31:484–489. doi: 10.1152/jappl.1971.31.3.484. [DOI] [PubMed] [Google Scholar]
- 9.Rajek A, Lenhardt R, Sessler DI, Grabenwöger M,JK, Mares P, Jantsch U, Gruber E. Tissue heat content and distribution during and after cardiopulmonary bypass at 17°C. Anesth Analg. 1999;88:1220–5. doi: 10.1097/00000539-199906000-00006. [DOI] [PubMed] [Google Scholar]
- 10.Rajek A, Lenhardt R, Sessler DI, Brunner G, Haisjackl M, Kastner J, Laufer G. Efficacy of two methods for reducing post-bypass afterdrop. Anesthesiology. 2000;92:447–456. doi: 10.1097/00000542-200002000-00027. [DOI] [PubMed] [Google Scholar]
- 11.Lenhardt R, Negishi C, Sessler DI, Ozaki M, Tayefeh F, Kurz A. Paralysis only slightly reduces the febrile response to interleukin-2 during isoflurane anesthesia. Anesthesiology. 1998;89:648–656. doi: 10.1097/00000542-199809000-00014. [DOI] [PubMed] [Google Scholar]
- 12.Rohrer K, Ali S, Taniguchi Y, Lenhardt R, Kurz A. Comparison of Heat Transfer Using Two Different Methods - Endovascular Versus Surface Cooling and Rewarming in Healthy Volunteers. Anesthesiology. 2004;101:A-538. [Google Scholar]
- 13.Belani K, Sessler DI, Sessler AM, Schroeder M, McGuire J, Merrifield B, Washington DE, Moayeri A. Leg heat content continues to decrease during the core temperature plateau in humans anesthetized with isoflurane. Anesthesiology. 1993;78:856–63. doi: 10.1097/00000542-199305000-00008. [DOI] [PubMed] [Google Scholar]
- 14.Fox RH, Solman AJ. A new technique for monitoring the deep body temperature in man from the intact skin surface. J Physiol (US) 1970;212:8–10. [PubMed] [Google Scholar]
- 15.Togawa T, Nemoto T, Yamazaki T, Kobayashi T. A modified internal temperature measurement device. Med Biol Eng. 1976;14:361–364. doi: 10.1007/BF02478138. [DOI] [PubMed] [Google Scholar]
- 16.Sessler DI, Schroeder M. Heat loss in humans covered with cotton hospital blankets. Anesth Analg. 1993;77:73–77. doi: 10.1213/00000539-199307000-00014. [DOI] [PubMed] [Google Scholar]
- 17.Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–310. [PubMed] [Google Scholar]
- 18.Wissler EH. Comparison of computed results obtained from two mathematical models - a simple 14-node model and a complex 250-node model. J Physiologie. 1971;63:455–458. [PubMed] [Google Scholar]
- 19.Matsukawa T, Kurz A, Sessler DI, Bjorksten AR, Merrifield B, Cheng C. Propofol linearly reduces the vasoconstriction and shivering thresholds. Anesthesiology. 1995;82:1169–1180. doi: 10.1097/00000542-199505000-00012. [DOI] [PubMed] [Google Scholar]
- 20.Romanovsky AA, Quint PA, Benikova Y, Kiesow LA. A difference of 5 degrees C between ear and rectal temperatures in a febrile patient. Am J Emerg Med. 1997;15:383–5. doi: 10.1016/s0735-6757(97)90133-9. [DOI] [PubMed] [Google Scholar]
- 21.Hayes JK, Collette DJ, Peters JL, Smith KW. Monitoring body-core temperature from the trachea: Comparison between pulmonary artery, tympanic, esophageal, and rectal temperatures. J Clin Monit. 1996;12:261–9. doi: 10.1007/BF00857648. [DOI] [PubMed] [Google Scholar]
- 22.Ash CJ, Cook JR, McMurry TA, Auner CR. The use of rectal temperature to monitor heat stroke. MO Med. 1992;89:283–288. [PubMed] [Google Scholar]