

Abstract
OBJECTIVE—The reflex sympathetic dystrophy syndrome (RSDS) is a painful limb disorder, for which a consistently effective treatment has not yet been identified. The disease is associated with increased bone resorption and patchy osteoporosis, which might benefit from treatment with bisphosphonates, powerful inhibitors of bone resorption. METHODS—Twenty patients with RSDS of foot and hand, were randomly assigned to blind administration of either alendronate intravenously (Istituto Gentili, Pisa, Italy) 7.5 mg dissolved in 250 ml saline solution or placebo saline infusions daily for three days. Two weeks later all patients had an identical treatment course with open labelled alendronate (7.5 mg/day for three days), independent from the results of the first blind treatment. RESULTS—In the patients treated with blind alendronate the diminution in spontaneous pain, tenderness, and swelling (circumference of the affected limb) and the improvement in motion were significantly different from baseline (p<0.001), from those observed within the first two weeks in the control group (p<0.01), and from week 2 to week 4 (p<0.01). In the patients given blind placebo infusions no relevant symptomatic changes were observed after the first two weeks of follow up, but they responded to the open alendronate therapy given afterwards. In 12 patients with RSDS of the hand the ultradistal bone mineral content (BMC) of the affected arm was considerably lower than that of the controlateral arm (mean (SD)) (426(82) mg/cm versus 688(49)). Six weeks after the beginning of the trial BMC rose by 77(12) mg/cm (p<0.001) in the affected arm, but it did not change in the controlateral. CONCLUSIONS—These results indicate that bisphosphonates should be considered for the treatment of RSDS, producing consistent and rapid remission of the disease.
Full Text
The Full Text of this article is available as a PDF (104.8 KB).
Figure 1 .

Changes in the circumference of the affected limbs (together with mean and standard deviation) two and four weeks after the beginning of the trial in the patients randomly assigned to either alendronate (right panel) or placebo (left panel) at the beginning of the study. At week 2 both groups of patients had a treatment course with intravenous alendronate.
Figure 2 .
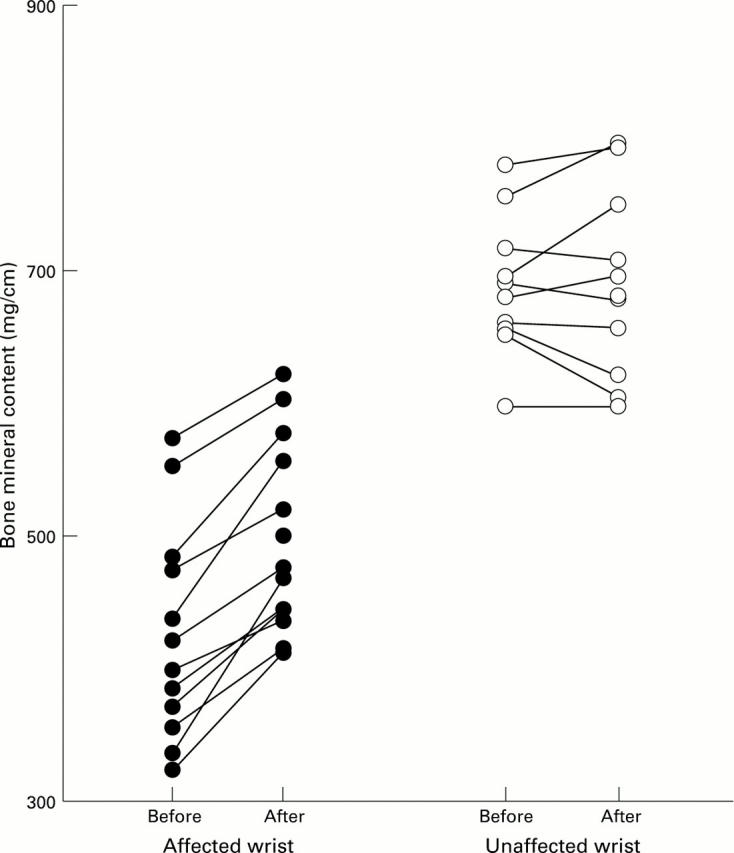
Changes in the bone mineral content of the wrist six weeks after the beginning of the trial in the RSDS affected and unaffected hand.