

Abstract
OBJECTIVES—To study the efficacy of allopurinol and benzbromarone to reduce serum urate concentrations in patients with primary chronic gout. METHODS—Prospective, parallel, open study of 86 consecutive male patients with primary chronic gout. Forty nine patients (26 normal excretors and 23 under excretors) were given allopurinol 300 mg/day and 37 under excretors benzbromarone 100 mg/day. After achieving steady plasma urate concentrations with such doses, treatment was then adjusted to obtain optimal plasmatic urate concentrations (under 6 mg/dl). RESULTS—Patients receiving allopurinol 300 mg/day showed a mean reduction of plasmatic urate of 2.75 mg/dl (from 8.60 to 5.85 mg/dl) and 3.34 mg/dl (from 9.10 to 5.76 mg/dl) in normal excretors and under excretors respectively. Patients receiving benzbromarone 100 mg/day achieved a reduction of plasmatic urate of 5.04 mg/dl (from 8.58 to 3.54 mg/dl). Fifty three per cent of patients receiving allopurinol and 100% receiving benzbromarone achieved optimal plasma urate concentrations at such doses. The patients with poor results with allopurinol 300 mg/day achieved a proper plasma urate concentration with allopurinol 450 to 600 mg/day, the mean final dose being 372 mg/day. Renal fuction improved and no case of renal lithiasis was observed among benzbromarone treated patients, whose mean final dose was 76 mg/day. CONCLUSION—Benzbromarone is very effective to control plasma urate concentrations at doses ranging from 50 to 100 mg/day. Uricosuric treatment is a suitable approach to the treatment of patients with gout who show underexcretion of urate. Keywords: gout; gout suppressants; allopurinol; benzbromarone
Full Text
The Full Text of this article is available as a PDF (120.9 KB).
Figure 1 .
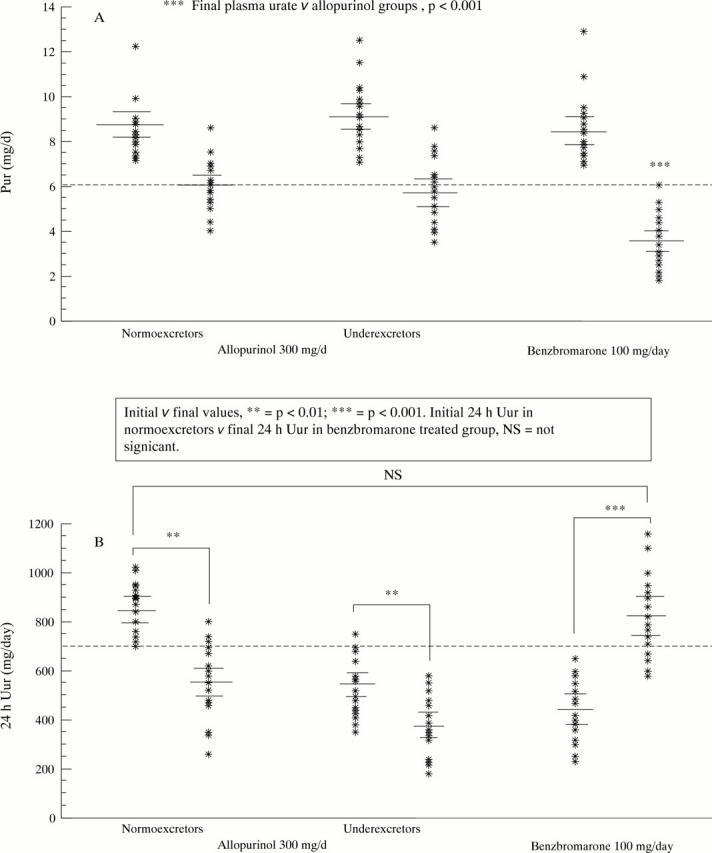
Initial and final plasma urate (Pur) (fig 1A) and 24 hour urinary urate (24 h Uur) (fig 1B) after standard doses of urate lowering drugs (allopurinol 300 mg/day or benzbromarone 100 mg/day). Note that the mean initial 24 h Uur in normoexcretors is not different to the mean final 24 h Uur from underexcretors treated with benzbromarone. Bars indicate the mean and the 95% confidence limits.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Asplin J. R. Uric acid stones. Semin Nephrol. 1996 Sep;16(5):412–424. [PubMed] [Google Scholar]
- Bellamy N., Gilbert J. R., Brooks P. M., Emmerson B. T., Campbell J. A survey of current prescribing practices of antiinflammatory and urate lowering drugs in gouty arthritis in the province of Ontario. J Rheumatol. 1988 Dec;15(12):1841–1847. [PubMed] [Google Scholar]
- Boss G. R., Seegmiller J. E. Hyperuricemia and gout. Classification, complications and management. N Engl J Med. 1979 Jun 28;300(26):1459–1468. doi: 10.1056/NEJM197906283002604. [DOI] [PubMed] [Google Scholar]
- Bull P. W., Scott J. T. Intermittent control of hyperuricemia in the treatment of gout. J Rheumatol. 1989 Sep;16(9):1246–1248. [PubMed] [Google Scholar]
- Cummins D., Sekar M., Halil O., Banner N. Myelosuppression associated with azathioprine-allopurinol interaction after heart and lung transplantation. Transplantation. 1996 Jun 15;61(11):1661–1662. doi: 10.1097/00007890-199606150-00023. [DOI] [PubMed] [Google Scholar]
- Cutrín Prieto C., Nieto Pol E., Batalla Eiras A., Casal Iglesias L., Pérez Becerra E., Lorenzo Zúiga V. Hepatitis tóxica por cincofeno: descripción de tres enfermos. Med Clin (Barc) 1991 Jun 15;97(3):104–106. [PubMed] [Google Scholar]
- Diamond H. S. Control of crystal-induced arthropathies. Rheum Dis Clin North Am. 1989 Aug;15(3):557–567. [PubMed] [Google Scholar]
- Emmerson B. T. The management of gout. N Engl J Med. 1996 Feb 15;334(7):445–451. doi: 10.1056/NEJM199602153340707. [DOI] [PubMed] [Google Scholar]
- Fam A. G. Should patients with interval gout be treated with urate lowering drugs? J Rheumatol. 1995 Sep;22(9):1621–1623. [PubMed] [Google Scholar]
- Fam A. G. Strategies and controversies in the treatment of gout and hyperuricaemia. Baillieres Clin Rheumatol. 1990 Aug;4(2):177–192. doi: 10.1016/s0950-3579(05)80016-0. [DOI] [PubMed] [Google Scholar]
- Ferraz M. B. An evidence based appraisal of the management of nontophaceous interval gout. J Rheumatol. 1995 Sep;22(9):1618–1619. [PubMed] [Google Scholar]
- Ferraz M. B., O'Brien B. A cost effectiveness analysis of urate lowering drugs in nontophaceous recurrent gouty arthritis. J Rheumatol. 1995 May;22(5):908–914. [PubMed] [Google Scholar]
- Fiddis R. W., Vlachos N., Calvert P. D. Studies of urate crystallisation in relation to gout. Ann Rheum Dis. 1983 Aug;42 (Suppl 1):12–15. doi: 10.1136/ard.42.suppl_1.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gast L. F. Reduce serum uric acid levels before withdrawing antihyperuricemic therapy in patients with tophaceous gout. Arthritis Rheum. 1992 Oct;35(10):1252–1252. doi: 10.1002/art.1780351024. [DOI] [PubMed] [Google Scholar]
- Gast L. F. Withdrawal of longterm antihyperuricemic therapy in tophaceous gout. Clin Rheumatol. 1987 Mar;6(1):70–73. doi: 10.1007/BF02201004. [DOI] [PubMed] [Google Scholar]
- Gehenot M., Horsmans Y., Rahier J., Geubel A. P. Subfulminant hepatitis requiring liver transplantation after benzarone administration. J Hepatol. 1994 Jun;20(6):842–842. doi: 10.1016/s0168-8278(05)80159-x. [DOI] [PubMed] [Google Scholar]
- Hande K. R., Noone R. M., Stone W. J. Severe allopurinol toxicity. Description and guidelines for prevention in patients with renal insufficiency. Am J Med. 1984 Jan;76(1):47–56. doi: 10.1016/0002-9343(84)90743-5. [DOI] [PubMed] [Google Scholar]
- Harris C. M., Lloyd D. C., Lewis J. The prevalence and prophylaxis of gout in England. J Clin Epidemiol. 1995 Sep;48(9):1153–1158. doi: 10.1016/0895-4356(94)00244-k. [DOI] [PubMed] [Google Scholar]
- Hautekeete M. L., Henrion J., Naegels S., DeNeve A., Adler M., Deprez C., Devis G., Klöppel G. Severe hepatotoxicity related to benzarone: a report of three cases with two fatalities. Liver. 1995 Feb;15(1):25–29. doi: 10.1111/j.1600-0676.1995.tb00102.x. [DOI] [PubMed] [Google Scholar]
- Kaehny W. D., Tangel D. J., Johnson A. M., Kimberling W. J., Schrier R. W., Gabow P. A. Uric acid handling in autosomal dominant polycystic kidney disease with normal filtration rates. Am J Med. 1990 Jul;89(1):49–52. doi: 10.1016/0002-9343(90)90097-w. [DOI] [PubMed] [Google Scholar]
- Loebl W. Y., Scott J. T. Withdrawal of allopurinol in patients with gout. Ann Rheum Dis. 1974 Jul;33(4):304–307. doi: 10.1136/ard.33.4.304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masbernard A., Giudicelli C. P. Ten years' experience with benzbromarone in the management of gout and hyperuricaemia. S Afr Med J. 1981 May 9;59(20):701–706. [PubMed] [Google Scholar]
- McCarthy G. M., Barthelemy C. R., Veum J. A., Wortmann R. L. Influence of antihyperuricemic therapy on the clinical and radiographic progression of gout. Arthritis Rheum. 1991 Dec;34(12):1489–1494. doi: 10.1002/art.1780341203. [DOI] [PubMed] [Google Scholar]
- Nakayama D. A., Barthelemy C., Carrera G., Lightfoot R. W., Jr, Wortmann R. L. Tophaceous gout: a clinical and radiographic assessment. Arthritis Rheum. 1984 Apr;27(4):468–471. doi: 10.1002/art.1780270417. [DOI] [PubMed] [Google Scholar]
- Nicholls A., Scott J. T. Effect of weight-loss on plasma and urinary levels of uric acid. Lancet. 1972 Dec 9;2(7789):1223–1224. doi: 10.1016/s0140-6736(72)92271-4. [DOI] [PubMed] [Google Scholar]
- Palella T. D., Kelley W. N. An approach to hyperuricemia and gout. Geriatrics. 1984 Nov;39(11):89-92, 95-6, 101-2. [PubMed] [Google Scholar]
- Puig J. G., Mateos F. A., Jiménez M. L., Ramos T. H. Renal excretion of hypoxanthine and xanthine in primary gout. Am J Med. 1988 Oct;85(4):533–537. doi: 10.1016/s0002-9343(88)80091-3. [DOI] [PubMed] [Google Scholar]
- Ralston S. H., Capell H. A., Sturrock R. D. Alcohol and response to treatment of gout. Br Med J (Clin Res Ed) 1988 Jun 11;296(6637):1641–1642. doi: 10.1136/bmj.296.6637.1641-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenthal A. K., Ryan L. M. Treatment of refractory crystal-associated arthritis. Rheum Dis Clin North Am. 1995 Feb;21(1):151–161. [PubMed] [Google Scholar]
- Simkin P. A. Management of gout. Ann Intern Med. 1979 May;90(5):812–816. doi: 10.7326/0003-4819-90-5-812. [DOI] [PubMed] [Google Scholar]
- Sinclair D. S., Fox I. H. The pharmacology of hypouricemic effect of benzbromarone. J Rheumatol. 1975 Dec;2(4):437–445. [PubMed] [Google Scholar]
- Singer J. Z., Wallace S. L. The allopurinol hypersensitivity syndrome. Unnecessary morbidity and mortality. Arthritis Rheum. 1986 Jan;29(1):82–87. doi: 10.1002/art.1780290111. [DOI] [PubMed] [Google Scholar]
- Sorensen L. B., Levinson D. J. Clinical evaluation of benzbromarone: a new uricosuric drug. Arthritis Rheum. 1976 Mar-Apr;19(2):183–190. doi: 10.1002/art.1780190209. [DOI] [PubMed] [Google Scholar]
- Wallace S. L., Robinson H., Masi A. T., Decker J. L., McCarty D. J., Yü T. F. Preliminary criteria for the classification of the acute arthritis of primary gout. Arthritis Rheum. 1977 Apr;20(3):895–900. doi: 10.1002/art.1780200320. [DOI] [PubMed] [Google Scholar]
- Wallace S. L., Singer J. Z. Therapy in gout. Rheum Dis Clin North Am. 1988 Aug;14(2):441–457. [PubMed] [Google Scholar]
- Walter-Sack I., de Vries J. X., von Bubnoff A., Pfleilschifter V., Raedsch R. Biotransformation and uric acid lowering effect of benzbromarone in patients with liver cirrhosis - evidence for active benzbromarone metabolites? Eur J Med Res. 1995 Oct 16;1(1):16–20. [PubMed] [Google Scholar]
- Wolfe F., Cathey M. A. The misdiagnosis of gout and hyperuricemia. J Rheumatol. 1991 Aug;18(8):1232–1234. [PubMed] [Google Scholar]
- Yü T., Yu T. F. Milestones in the treatment of gout. Am J Med. 1974 May;56(5):676–685. doi: 10.1016/0002-9343(74)90634-2. [DOI] [PubMed] [Google Scholar]
- Zürcher R. M., Bock H. A., Thiel G. Excellent uricosuric efficacy of benzbromarone in cyclosporin-A-treated renal transplant patients: a prospective study. Nephrol Dial Transplant. 1994;9(5):548–551. doi: 10.1093/ndt/9.5.548. [DOI] [PubMed] [Google Scholar]
- van Lieshout-Zuidema M. F., Breedveld F. C. Withdrawal of longterm antihyperuricemic therapy in tophaceous gout. J Rheumatol. 1993 Aug;20(8):1383–1385. [PubMed] [Google Scholar]
- van der Klauw M. M., Houtman P. M., Stricker B. H., Spoelstra P. Hepatic injury caused by benzbromarone. J Hepatol. 1994 Mar;20(3):376–379. doi: 10.1016/s0168-8278(94)80011-1. [DOI] [PubMed] [Google Scholar]