

Abstract
OBJECTIVES—To study benefits and skeletal side effects of carefully monitored prednisolone treatment in patients with active rheumatoid arthritis. METHODS—One hundred and two patients with active rheumatoid arthritis were randomly allocated to treatment with disease modifying anti-inflammatory drug (DMARD) alone or DMARD and prednisolone in a one year follow up study. Prednisolone was given in a dose regimen adapted to the disease activity of the individual patient. The mean dose was 6 mg and the mean cumulated dose was 2160 mg. Patients were followed up with disease activity parameters, radiograph of the hands (Larsen score), and bone mineral density (BMD) of the lumbar spine, distal forearm and hand. At one year 26 patients had withdrawn from the investigation leaving 76 patients for evaluation. RESULTS—The results showed that disease activity in the prednisolone treated group was reduced within two weeks. In the DMARD alone group disease activity was gradually reduced over months. At six months there was no difference between the groups as evaluated by an improvement score using a number of ACR criteria. Prednisolone in the present set up was not able to protect significantly against radiological disease progression, although there was a trend towards less progression in Larsen score in the prednisolone group, a matter that was further underlined in an intention to treat analysis. BMD data revealed a significant reduction in spinal BMD in the prednisolone group, whereas prednisolone seemed to have a protective effect against bone loss in the hand and distal forearm. CONCLUSIONS—This study does not allow any firm conclusions for or against the treatment of rheumatoid arthritis with prednisolone. The data suggest that the beneficial effects of prednisolone are not as clear cut in established rheumatoid arthritis as in early disease. Furthermore the data indicate that treatment in the chosen relatively low dose does not provide sufficient control of disease. On the other hand the spinal bone loss observed in the prednisolone group does invite considerations about using higher doses.
Full Text
The Full Text of this article is available as a PDF (79.7 KB).
Figure 1 .

A CONSORT flow diagram to show patient courses during the study.
Figure 2 .
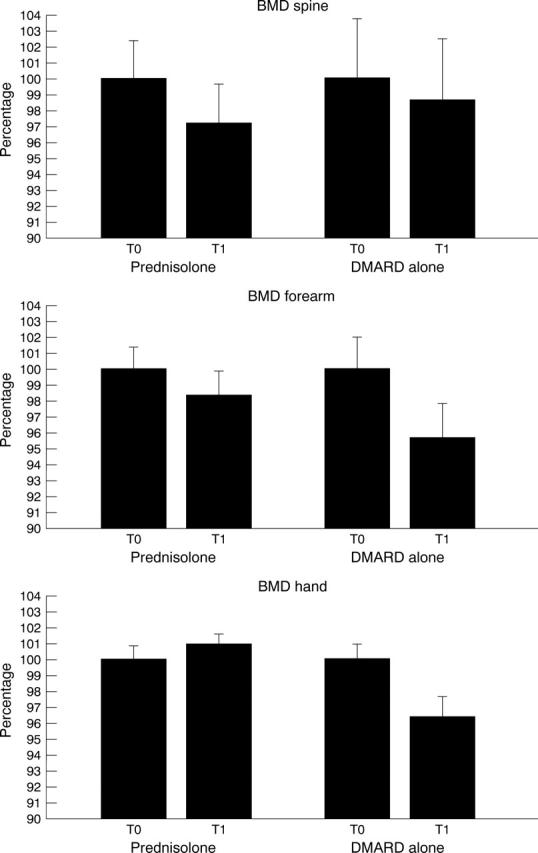
Changes in bone mineral density (BMD) of the lumbar spine, distal forearm, and hand during one year of treatment with DMARD alone or DMARD + prednisolone. The values at T-start are set at 100% and values at T-1 year are given in per cent of the starting value. Bars indicate standard error of the mean (SEM %).
Figure 3 .
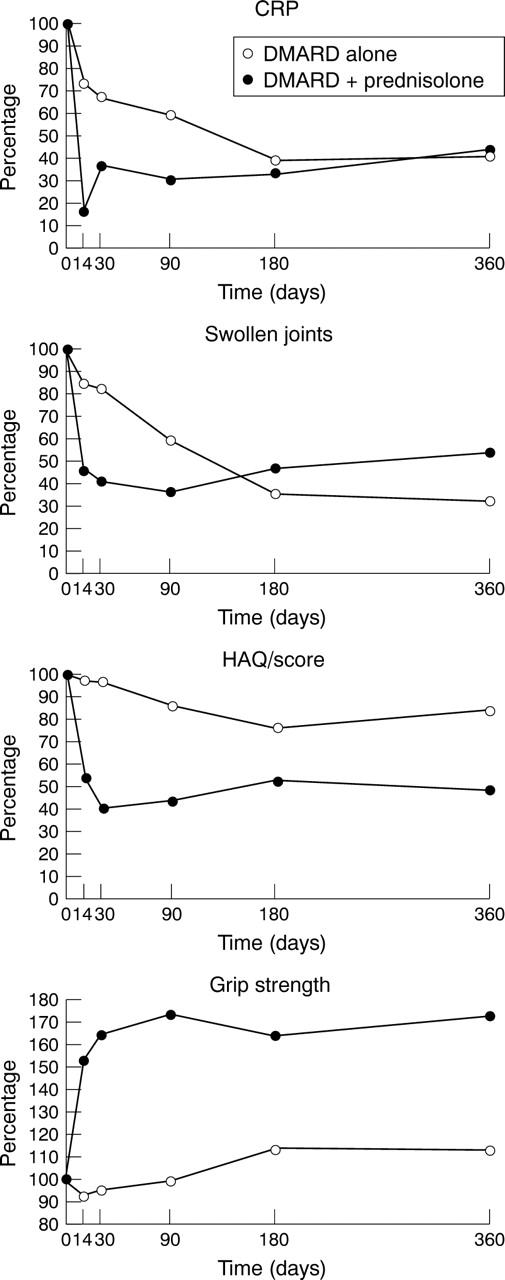
Changes in clinical and biochemical variables of disease activity during one year of treatment with DMARD alone or DMARD + prednisolone. HAQ = Health Assessment Questionnaire.CRP = C reactive protein. Data are shown as mean % of T-start.