

Abstract
OBJECTIVE—KL-6 is a mucin-like high molecular weight glycoprotein, which is strongly expressed on type II alveolar pneumocytes and bronchiolar epithelial cells. It has been demonstrated that the KL-6 antigen is a useful marker for estimating the activity of interstitial pneumonia. In this study, it is hypothesised that serum KL-6 is a useful marker to evaluate the activity of interstitial pneumonia associated with polymyositis/dermatomyositis (PM/DM). METHODS—KL-6 was measured in sera in 16 patients diagnosed with PM/DM. Five had non-specific interstitial pneumonia (NSIP), three had diffuse alveolar damage (DAD), and eight had no pulmonary involvement, and 10 were normal non-smokers as a control group. The correlation was also evaluated between the KL-6 level and each clinical course in patients with pulmonary involvement associated with PM/DM. Immunohistochemical analysis using monoclonal anti-KL-6 antibody was also performed. RESULTS—KL-6 concentrations in sera of patients with interstitial pneumonia associated with PM/DM were significantly high compared with those of PM/DM without interstitial pneumonia, and normal non-smokers. KL-6 concentrations in sera in patients with DAD significantly increased compared with those of other groups. KL-6 values in sera changed according to the progression or improvement of interstitial pneumonia. Immunohistochemical study using pulmonary tissues obtained from patients with DAD demonstrated that the hyaline membrane, proliferating type II pneumocytes, bronchial epithelial cells and some endothelial cells in pulmonary veins were stained by antihuman KL-6 antibody. CONCLUSION—These data demonstrate that measurement of serum KL-6 was a useful marker to evaluate the activity of acute interstitial pneumonia associated with PM/DM.
Full Text
The Full Text of this article is available as a PDF (172.4 KB).
Figure 1 .
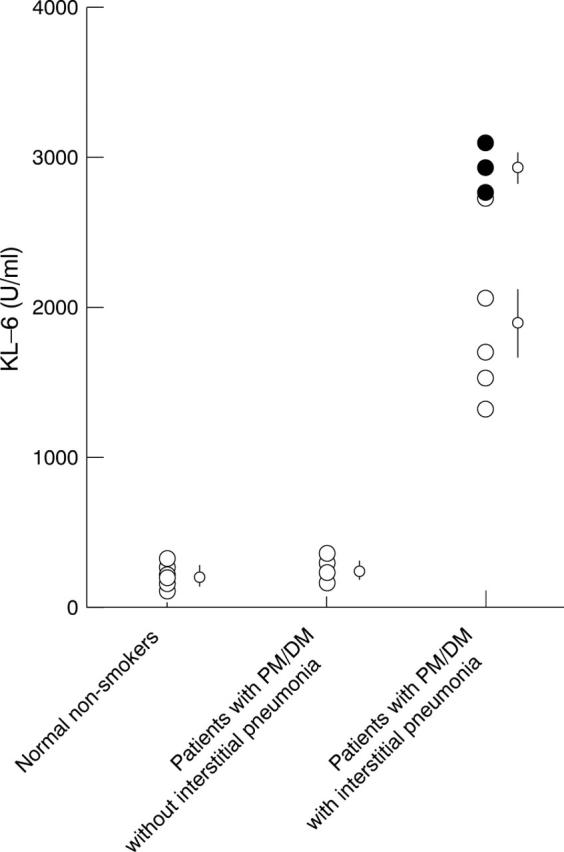
Serum KL-6 concentrations in normal non-smokers, patients with PM/DM without interstitial pneumonia and patients with PM/DM with interstitial pneumonia (non-specific interstitial pneumonia (NIP, empty circles), and patients with diffuse alveolar damage (DAD, black circles)). Bars represent mean (SEM).
Figure 2 .

Changes of serum KL-6 concentrations according to clinical courses in six patients with PM/DM with interstitial pneumonia. Progression or improvement of the disease was determined by PaO2 values, pulmonary function tests, and changes of chest computed tomographic findings one month after treatment. (A) Progressed cases (two patients), (B) improved cases (four patients).
Figure 3 .
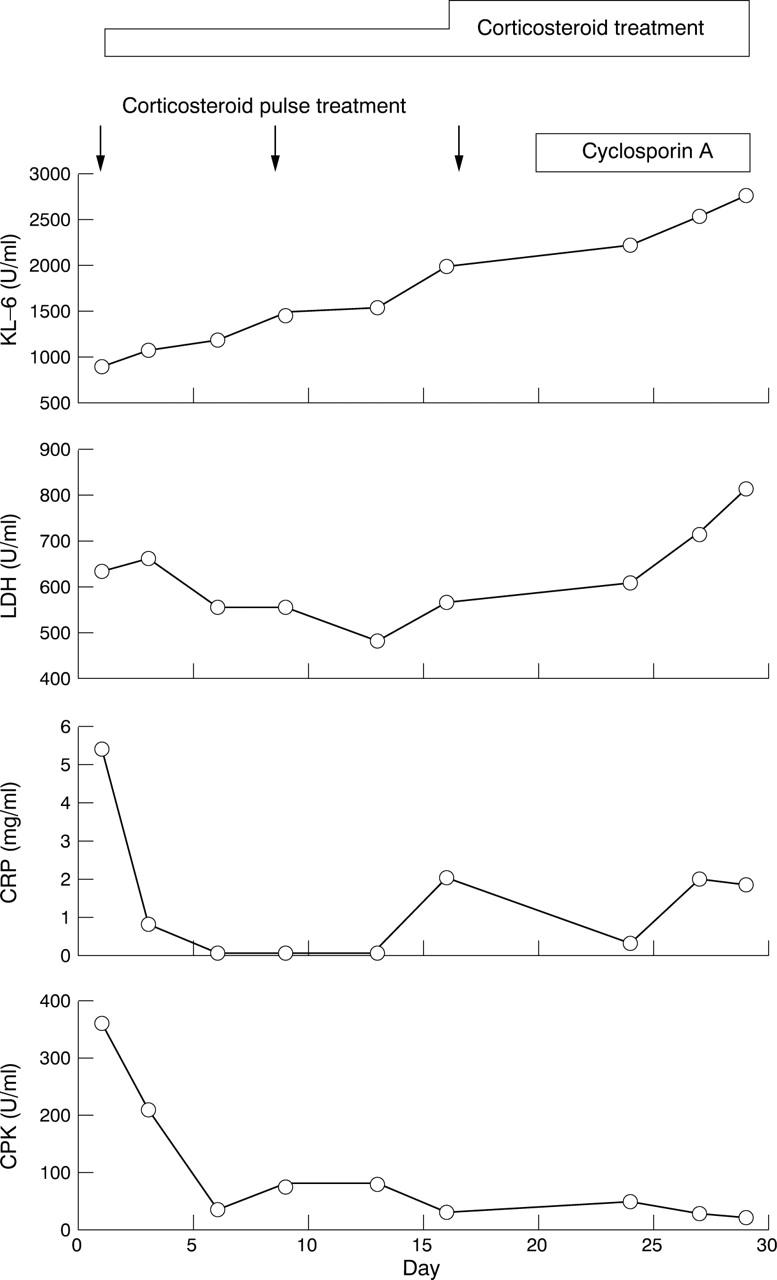
Changes of serum KL-6, lactate dehydrogenase (LDH), C reactive protein (CRP) and creatine phosphokinase (CPK) values according to clinical courses in a patient (patient number 1 in table 1) with PM/DM complicated with interstitial pneumonia (DAD). This case did not respond to the immunosuppressive treatment at all. The clinical course was reflected in the sequential changes of KL-6.
Figure 4 .

The distribution of KL-6 antigen in lung tissue sections from patients with DAD was examined by means of immunoperoxidase staining and counterstained with haematoxylin. (A) Lung section featuring DAD; KL-6 antibody reacted moderately with the hyaline membrane (arrows). (B) Lung section exhibiting fibrotic change; KL-6 antibody reacted strongly with regenerating type II pneumocytes (arrows), especially their apical parts, but did not react with interstitial components. (C) Under high magnification of the hyaline membrane staining (large arrow), was less dense compared with the surrounding type II pneumocytes (arrowheads) and the content in the narrowed airspase (small arrows). (D) Some endothelial cells in pulmonary veins were also stained by this antibody (arrow heads) as well as bronchiolar epithelial cells (small arrows). The labelled streptavidin biotin peroxidase (LSABC) method was used. (A: original magnification ×90; B, C, D: original magnification ×180).
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bohan A., Peter J. B. Polymyositis and dermatomyositis (first of two parts). N Engl J Med. 1975 Feb 13;292(7):344–347. doi: 10.1056/NEJM197502132920706. [DOI] [PubMed] [Google Scholar]
- Hamada H., Kohno N., Akiyama M., Hiwada K. Monitoring of serum KL-6 antigen in a patient with radiation pneumonia. Chest. 1992 Mar;101(3):858–860. doi: 10.1378/chest.101.3.858. [DOI] [PubMed] [Google Scholar]
- Katzenstein A. L., Fiorelli R. F. Nonspecific interstitial pneumonia/fibrosis. Histologic features and clinical significance. Am J Surg Pathol. 1994 Feb;18(2):136–147. [PubMed] [Google Scholar]
- Katzenstein A. L., Myers J. L., Mazur M. T. Acute interstitial pneumonia. A clinicopathologic, ultrastructural, and cell kinetic study. Am J Surg Pathol. 1986 Apr;10(4):256–267. [PubMed] [Google Scholar]
- Kobayashi J., Kitamura S. KL-6: a serum marker for interstitial pneumonia. Chest. 1995 Aug;108(2):311–315. doi: 10.1378/chest.108.2.311. [DOI] [PubMed] [Google Scholar]
- Kobayashi J., Kitamura S. Serum KL-6 for the evaluation of active pneumonitis in pulmonary sarcoidosis. Chest. 1996 May;109(5):1276–1282. doi: 10.1378/chest.109.5.1276. [DOI] [PubMed] [Google Scholar]
- Kohno N., Akiyama M., Kyoizumi S., Hakoda M., Kobuke K., Yamakido M. Detection of soluble tumor-associated antigens in sera and effusions using novel monoclonal antibodies, KL-3 and KL-6, against lung adenocarcinoma. Jpn J Clin Oncol. 1988 Sep;18(3):203–216. [PubMed] [Google Scholar]
- Kohno N., Akiyama M., Kyoizumi S., Tanabe M., Oyama T., Yamakido M. A novel method for screening monoclonal antibodies reacting with antigenic determinants on soluble antigens; a reversed indirect-enzyme linked immunosorbent assay (RI-ELISA). Hiroshima J Med Sci. 1987 Dec;36(4):319–323. [PubMed] [Google Scholar]
- Kohno N., Awaya Y., Oyama T., Yamakido M., Akiyama M., Inoue Y., Yokoyama A., Hamada H., Fujioka S., Hiwada K. KL-6, a mucin-like glycoprotein, in bronchoalveolar lavage fluid from patients with interstitial lung disease. Am Rev Respir Dis. 1993 Sep;148(3):637–642. doi: 10.1164/ajrccm/148.3.637. [DOI] [PubMed] [Google Scholar]
- Kohno N., Hamada H., Fujioka S., Hiwada K., Yamakido M., Akiyama M. Circulating antigen KL-6 and lactate dehydrogenase for monitoring irradiated patients with lung cancer. Chest. 1992 Jul;102(1):117–122. doi: 10.1378/chest.102.1.117. [DOI] [PubMed] [Google Scholar]
- Kohno N., Kyoizumi S., Awaya Y., Fukuhara H., Yamakido M., Akiyama M. New serum indicator of interstitial pneumonitis activity. Sialylated carbohydrate antigen KL-6. Chest. 1989 Jul;96(1):68–73. doi: 10.1378/chest.96.1.68. [DOI] [PubMed] [Google Scholar]
- MILLS E. S., MATHEWS W. H. Interstitial pneumonitis in dermatomyositis. J Am Med Assoc. 1956 Apr 28;160(17):1467–1470. doi: 10.1001/jama.1956.02960520029008b. [DOI] [PubMed] [Google Scholar]
- Tazelaar H. D., Viggiano R. W., Pickersgill J., Colby T. V. Interstitial lung disease in polymyositis and dermatomyositis. Clinical features and prognosis as correlated with histologic findings. Am Rev Respir Dis. 1990 Mar;141(3):727–733. doi: 10.1164/ajrccm/141.3.727. [DOI] [PubMed] [Google Scholar]