

Abstract
Objective: To report a case of juvenile CNS-SLE, in which magnetic resonance imaging (MRI) was used to assess disease activity.
Case report: A 10 year old female patient with SLE presented with convulsions; MRI and computed tomography (CT) of the cerebrum disclosed abnormalities. Despite adequate treatment, two years later she had a generalised convulsion, and MRI showed new lesions. MR spectroscopy (MRS) indicated neuronal loss, inflammation, and metabolically compromised tissue; magnetisation transfer imaging (MTI) showed an increase in whole brain lesion load. After exclusion of a malignancy, CNS-SLE was the most likely diagnosis, and cyclophosphamide pulses were administered. Initially, multiple sclerosis (MS)-like lesions regressed, but despite maximal immunosuppressive drugs, new lesions formed and disappeared. When immunosuppressive drugs had been stopped for six months MRI showed improved lesions and MTI histograms.
Discussion: In this case report, the anatomical substrate, metabolic aspect, neuroimaging, and clinical course of MS-like lesions in a child with CNS-SLE are described. The way in which radiological techniques can support clinical decision making in this young patient with progressive CNS-SLE is illustrated.
Full Text
The Full Text of this article is available as a PDF (176.9 KB).
Figure 1.
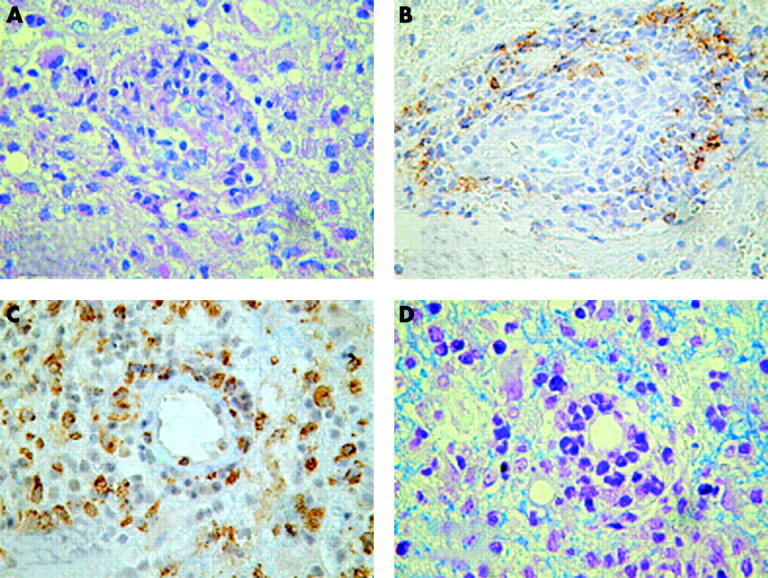
Histopathology of the brain tissue obtained by stereotactic surgery. (A) A mixed granulocytic and lymphocytic inflammatory reaction affecting the vessel walls is seen. The inflammatory response is non-specific. (Periodic acid-Schiff staining, x400). (B) Among the population of mononuclear cells the B lymphocytes are immunopositive for the B cell-specific marker CD20 (x400). (C) Among the inflammatory cells many activated microglial cells are seen (immunohistochemistry for CD56; x400). (D) The neuropilem shows oedema, but there are no signs of myelin-breakdown (Kluwer stain, x400).
Figure 2.

Fluid attenuated inversion recovery (FLAIR) images and MRS results of the occipitoparietal lesion and contralateral normal appearing white matter (NAWM), shortly after the generalised convulsion (active) and eight months later during clinical quiescent remission state (remission), when the patient was receiving pulses of cyclophosphamide. In the active state, the increased choline (Cho) and decreased N-acetyl-aspartate (NAA) peaks of the lesion indicate some degree of inflammation and neuronal damage. Also indicated are the creatine (Cre) peak and the double negative peak to the right side of the NAA peak, showing the presence of lactate (Lac), originating from metabolically compromised tissue. In remission, qualitative MR images show clear regression of the lesion, with normalisation of MRS metabolites (lactate no longer visible).