

Full Text
The Full Text of this article is available as a PDF (117.1 KB).
Figure 1.

Case 1. (A) Chest x ray findings show bibasilar reticular opacities, cardiomegaly with accentuation of the right ventricle, and enlargement of the pulmonary artery, which are consistent with interstitial lung disease and pulmonary hypertension. (B) High resolution CT of the lungs discloses features of interstitial lung disease with "ground glass" opacities and widening of the central blood vessels. (C) Doppler echocardiography shows blood regurgitation through the tricuspid valve, which allows estimation of PASP. (D) Perfusion scintigraphy of the lungs carried out in February 2000 (D/1) shows redistribution of the blood flow into the upper parts of the lungs and irregular areas of diminished blood flow in the peripheral parts of the lungs consistent with PAH and pulmonary thromboembolism. For comparison, perfusion scintigraphy of the lungs carried out in June 2000 (D/2) shows a significant increase in blood flow in the lower parts of both lungs, which paralleled a decrease in PASP as measured with Doppler echocardiography.
Figure 2.
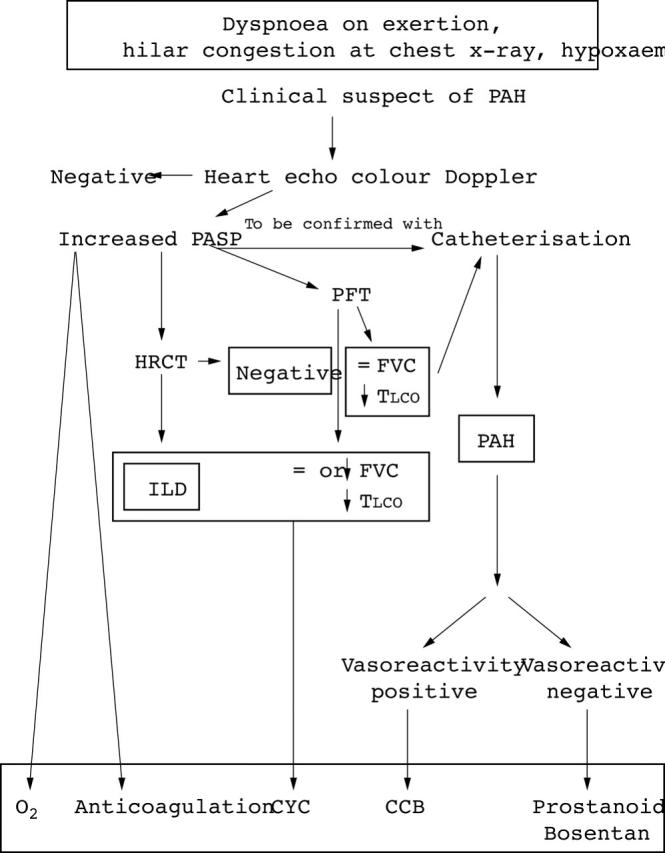
The flow chart suggests the diagnostic procedure and the possible therapeutic options for PAH in SSc. PASP, pulmonary artery systolic pressure; PFT, pulmonary function tests; TLCO, carbon monoxide transfer factor; FVC, forced vital capacity; CCB, calcium channel blockers; ILD, interstitial lung disease; HRCT, high resolution computed tomography; CYC, cyclophosphamide; PAH, pulmonary arterial hypertension.