

Abstract
OBJECTIVE—To assess and compare the safety and efficacy of amiodarone and sotalol in the treatment of patients with recurrent symptomatic atrial fibrillation. DESIGN—Prospective, randomised, single blind, placebo controlled study. SETTING—Tertiary cardiac referral centre. PATIENTS—186 consecutive patients (97 men, 89 women; mean (SD) age, 63 (10) years) with recurrent, symptomatic atrial fibrillation. INTERVENTIONS—65 patients were randomised to amiodarone, 61 to sotalol, and 60 to placebo. Patients receiving amiodarone were maintained at a dose of 200 mg/day after a 30 day loading phase. The sotalol dose was 160-480 mg daily, as tolerated. MAIN OUTCOME MEASURES—Recurrence of atrial fibrillation or side effects. RESULTS—In the amiodarone group, 31 of the 65 patients developed atrial fibrillation after an average of six months, while 15 (11 in sinus rhythm and four in atrial fibrillation) experienced significant side effects after an average of 16 months. In the sotalol group, relapse to atrial fibrillation occurred in 47 of the 61 patients after an average of eight months; three experienced side effects during the titration phase. In the placebo group, 53 of the 60 patients developed atrial fibrillation after an average of four months (p < 0.001 for amiodarone and sotalol v placebo; p < 0.001 for amiodarone v sotalol). CONCLUSIONS—Both amiodarone and sotalol can be used for the maintenance of normal sinus rhythm in patients with symptomatic atrial fibrillation. Amiodarone is more effective but causes more side effects. Keywords: amiodarone; sotalol; atrial fibrillation
Full Text
The Full Text of this article is available as a PDF (140.2 KB).
Figure 1 .
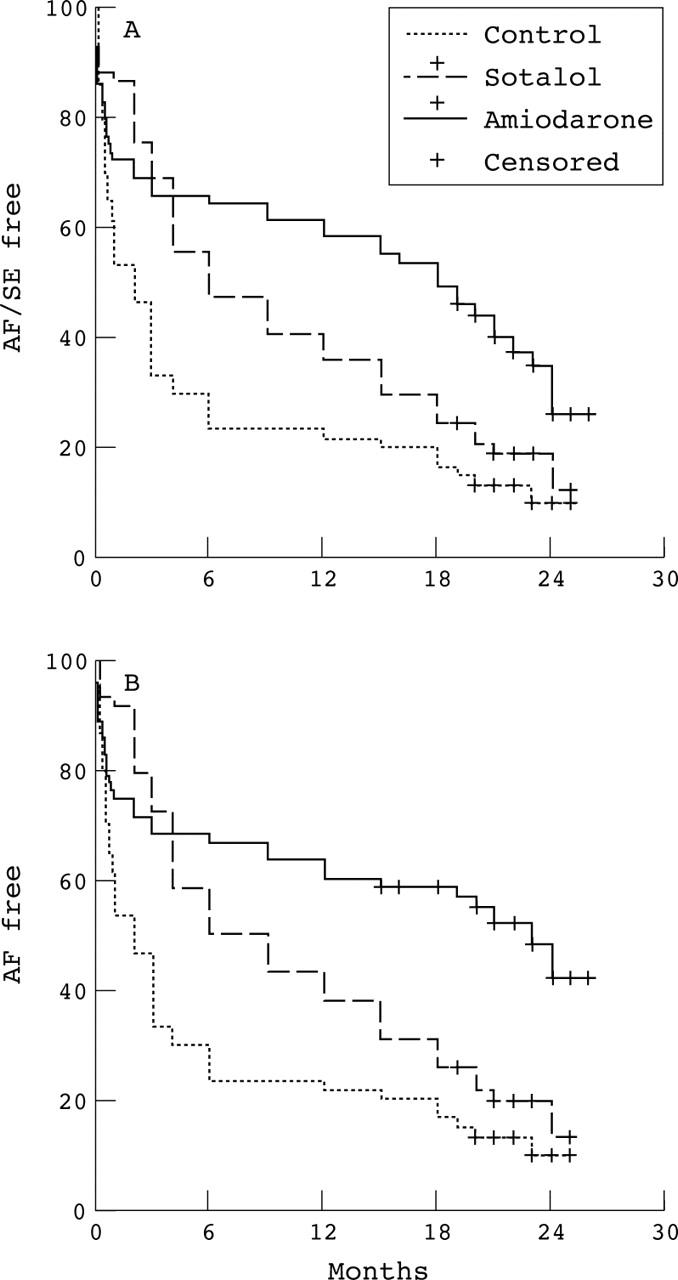
Kaplan-Meier curves for (A) the primary analysis and (B) the secondary analysis. Amiodarone and sotalol were superior to placebo. Amiodarone was better than sotalol, but its superiority only became evident after the six month point. When adverse effects are overlooked, amiodarone was seen to be much more effective than the other two agents. There was no difference in the pattern of censoring between the three groups. AF, atrial fibrillation; SE, side effects.
Figure 2 .
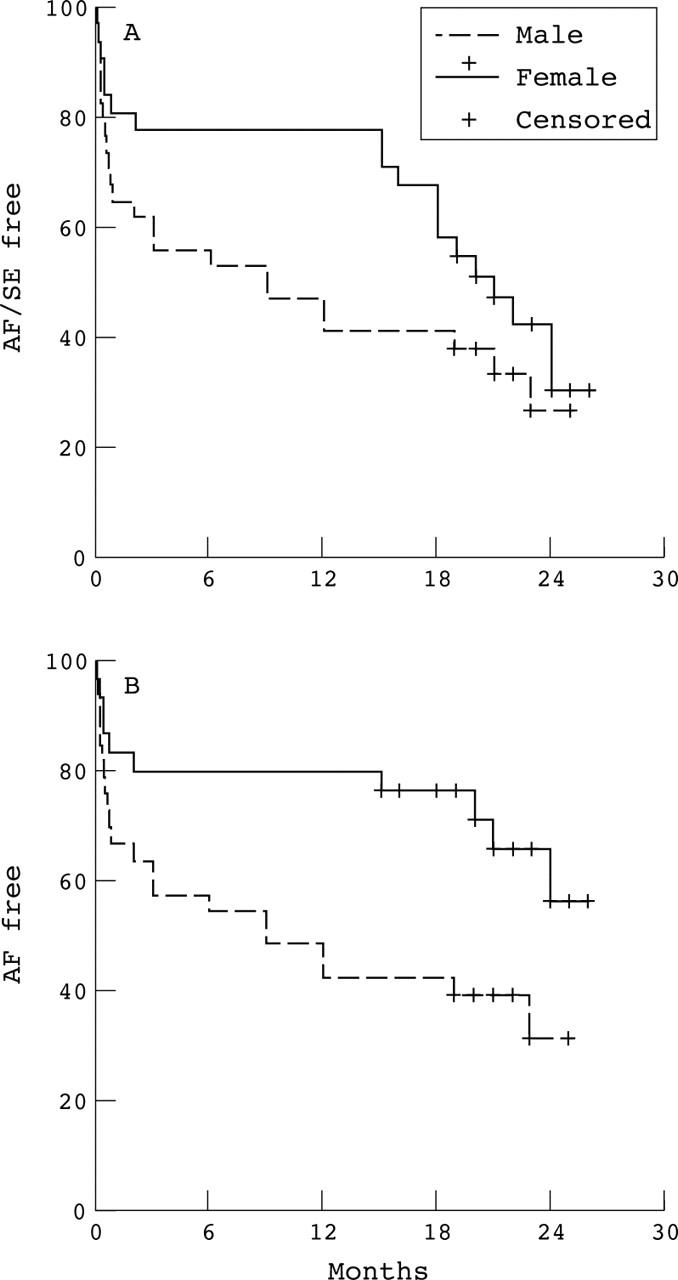
Kaplan-Meier curves for (A) the primary analysis, and (B) the secondary analysis, grouped by sex in the amiodarone group. Female patients had a much better chance of remaining in sinus rhythm for a longer period, but also experienced more side effects than men.
Figure 3 .

Progression to atrial fibrillation and side effects, with the first month's relapses censored. Amiodarone is now superior to sotalol throughout the period of observation.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Antman E. M., Beamer A. D., Cantillon C., McGowan N., Friedman P. L. Therapy of refractory symptomatic atrial fibrillation and atrial flutter: a staged care approach with new antiarrhythmic drugs. J Am Coll Cardiol. 1990 Mar 1;15(3):698–707. doi: 10.1016/0735-1097(90)90649-a. [DOI] [PubMed] [Google Scholar]
- Antman E. M., Ludmer P. L., McGowan N., Bosak M., Friedman P. L. Transtelephonic electrocardiographic transmission for management of cardiac arrhythmias. Am J Cardiol. 1986 Nov 1;58(10):1021–1024. doi: 10.1016/s0002-9149(86)80031-5. [DOI] [PubMed] [Google Scholar]
- Benditt D. G., Williams J. H., Jin J., Deering T. F., Zucker R., Browne K., Chang-Sing P., Singh B. N. Maintenance of sinus rhythm with oral d,l-sotalol therapy in patients with symptomatic atrial fibrillation and/or atrial flutter. d,l-Sotalol Atrial Fibrillation/Flutter Study Group. Am J Cardiol. 1999 Aug 1;84(3):270–277. doi: 10.1016/s0002-9149(99)00275-1. [DOI] [PubMed] [Google Scholar]
- Chimienti M., Cullen M. T., Jr, Casadei G. Safety of flecainide versus propafenone for the long-term management of symptomatic paroxysmal supraventricular tachyarrhythmias. Report from the Flecainide and Propafenone Italian Study (FAPIS) Group. Eur Heart J. 1995 Dec;16(12):1943–1951. doi: 10.1093/oxfordjournals.eurheartj.a060852. [DOI] [PubMed] [Google Scholar]
- Chun S. H., Sager P. T., Stevenson W. G., Nademanee K., Middlekauff H. R., Singh B. N. Long-term efficacy of amiodarone for the maintenance of normal sinus rhythm in patients with refractory atrial fibrillation or flutter. Am J Cardiol. 1995 Jul 1;76(1):47–50. doi: 10.1016/s0002-9149(99)80799-1. [DOI] [PubMed] [Google Scholar]
- Coplen S. E., Antman E. M., Berlin J. A., Hewitt P., Chalmers T. C. Efficacy and safety of quinidine therapy for maintenance of sinus rhythm after cardioversion. A meta-analysis of randomized control trials. Circulation. 1990 Oct;82(4):1106–1116. doi: 10.1161/01.cir.82.4.1106. [DOI] [PubMed] [Google Scholar]
- Edvardsson N. Comparison of class I and class III action in atrial fibrillation. Eur Heart J. 1993 Nov;14 (Suppl H):62–66. doi: 10.1093/eurheartj/14.suppl_h.62. [DOI] [PubMed] [Google Scholar]
- Gold R. L., Haffajee C. I., Charos G., Sloan K., Baker S., Alpert J. S. Amiodarone for refractory atrial fibrillation. Am J Cardiol. 1986 Jan 1;57(1):124–127. doi: 10.1016/0002-9149(86)90964-1. [DOI] [PubMed] [Google Scholar]
- Harjai K. J., Licata A. A. Effects of amiodarone on thyroid function. Ann Intern Med. 1997 Jan 1;126(1):63–73. doi: 10.7326/0003-4819-126-1-199701010-00009. [DOI] [PubMed] [Google Scholar]
- Hohnloser S. H., Meinertz T., Dammbacher T., Steiert K., Jähnchen E., Zehender M., Fraedrich G., Just H. Electrocardiographic and antiarrhythmic effects of intravenous amiodarone: results of a prospective, placebo-controlled study. Am Heart J. 1991 Jan;121(1 Pt 1):89–95. doi: 10.1016/0002-8703(91)90960-p. [DOI] [PubMed] [Google Scholar]
- Jafari-Fesharaki M., Scheinman M. M. Adverse effects of amiodarone. Pacing Clin Electrophysiol. 1998 Jan;21(1 Pt 1):108–120. doi: 10.1111/j.1540-8159.1998.tb01068.x. [DOI] [PubMed] [Google Scholar]
- Juul-Möller S., Edvardsson N., Rehnqvist-Ahlberg N. Sotalol versus quinidine for the maintenance of sinus rhythm after direct current conversion of atrial fibrillation. Circulation. 1990 Dec;82(6):1932–1939. doi: 10.1161/01.cir.82.6.1932. [DOI] [PubMed] [Google Scholar]
- Kochiadakis G. E., Igoumenidis N. E., Marketou M. E., Solomou M. C., Kanoupakis E. M., Vardas P. E. Low-dose amiodarone versus sotalol for suppression of recurrent symptomatic atrial fibrillation. Am J Cardiol. 1998 Apr 15;81(8):995–998. doi: 10.1016/s0002-9149(98)00078-2. [DOI] [PubMed] [Google Scholar]
- Nattel S. Newer developments in the management of atrial fibrillation. Am Heart J. 1995 Nov;130(5):1094–1106. doi: 10.1016/0002-8703(95)90214-7. [DOI] [PubMed] [Google Scholar]
- Porterfield J. G., Porterfield L. M. Therapeutic efficacy and safety of oral propafenone for atrial fibrillation. Am J Cardiol. 1989 Jan 1;63(1):114–116. doi: 10.1016/0002-9149(89)91091-6. [DOI] [PubMed] [Google Scholar]
- Prystowsky E. N., Benson D. W., Jr, Fuster V., Hart R. G., Kay G. N., Myerburg R. J., Naccarelli G. V., Wyse D. G. Management of patients with atrial fibrillation. A Statement for Healthcare Professionals. From the Subcommittee on Electrocardiography and Electrophysiology, American Heart Association. Circulation. 1996 Mar 15;93(6):1262–1277. doi: 10.1161/01.cir.93.6.1262. [DOI] [PubMed] [Google Scholar]
- Reimold S. C. Clinical challenge. I: Control of recurrent symptomatic atrial fibrillation. Eur Heart J. 1996 Jul;17 (Suppl 100):35–40. doi: 10.1093/eurheartj/17.suppl_c.35. [DOI] [PubMed] [Google Scholar]
- Rotmensch H. H., Belhassen B., Swanson B. N., Shoshani D., Spielman S. R., Greenspon A. J., Greenspan A. M., Vlasses P. H., Horowitz L. N. Steady-state serum amiodarone concentrations: relationships with antiarrhythmic efficacy and toxicity. Ann Intern Med. 1984 Oct;101(4):462–469. doi: 10.7326/0003-4819-101-4-462. [DOI] [PubMed] [Google Scholar]
- Scheinman M. M., Levine J. H., Cannom D. S., Friehling T., Kopelman H. A., Chilson D. A., Platia E. V., Wilber D. J., Kowey P. R. Dose-ranging study of intravenous amiodarone in patients with life-threatening ventricular tachyarrhythmias. The Intravenous Amiodarone Multicenter Investigators Group. Circulation. 1995 Dec 1;92(11):3264–3272. doi: 10.1161/01.cir.92.11.3264. [DOI] [PubMed] [Google Scholar]
- Singh B. N., Ahmed R. Class III antiarrhythmic drugs. Curr Opin Cardiol. 1994 Jan;9(1):12–22. doi: 10.1097/00001573-199401000-00003. [DOI] [PubMed] [Google Scholar]
- Southworth M. R., Zarembski D., Viana M., Bauman J. Comparison of sotalol versus quinidine for maintenance of normal sinus rhythm in patients with chronic atrial fibrillation. Am J Cardiol. 1999 Jun 15;83(12):1629–1632. doi: 10.1016/s0002-9149(99)00168-x. [DOI] [PubMed] [Google Scholar]
- Suttorp M. J., Kingma J. H., Koomen E. M., van 't Hof A., Tijssen J. G., Lie K. I. Recurrence of paroxysmal atrial fibrillation or flutter after successful cardioversion in patients with normal left ventricular function. Am J Cardiol. 1993 Mar 15;71(8):710–713. doi: 10.1016/0002-9149(93)91015-a. [DOI] [PubMed] [Google Scholar]
- Wang J., Bourne G. W., Wang Z., Villemaire C., Talajic M., Nattel S. Comparative mechanisms of antiarrhythmic drug action in experimental atrial fibrillation. Importance of use-dependent effects on refractoriness. Circulation. 1993 Sep;88(3):1030–1044. doi: 10.1161/01.cir.88.3.1030. [DOI] [PubMed] [Google Scholar]