

Abstract
Aims: To review the clinical presentation, radiographic findings, and outcome of therapy in children with septic pulmonary embolism.
Methods: Retrospective analysis of patients in a tertiary paediatric facility in northern Taiwan.
Results: Ten children were identified with septic pulmonary emboli in a four year retrospective chart review between 1998 and 2001. Seven were immunocompetent, two were premature infants, one had ß thalassemia major. Seven had community acquired staphylococcal infections and bacteraemia, of which six were methicillin resistant Staphylococus aureus (MRSA) isolates. Five had soft tissue infections, two bone infections, one suppurative otitis media, one catheter related infection, and one unknown foci of infection. Multiple and bilateral nodular pulmonary parenchymal lesions were common on plain chest radiographs, but chest computed tomography scans showed the additional findings of a "vessel sign" and central cavitations, confirming the existence of septic pulmonary embolism.
Conclusions: Community acquired MRSA infections occurred in seven patients with septic pulmonary embolism but without predisposing high risk factors. Critically ill children with skin, soft tissue, or bone infections, when associated with septic pulmonary embolism in an area with a high rate of MRSA, should be empirically treated with glycopeptides (such as vancomycin or teicoplanin) before susceptibility results are known, in order to minimise morbidity and avoid mortality.
Full Text
The Full Text of this article is available as a PDF (137.0 KB).
Figure 1 .
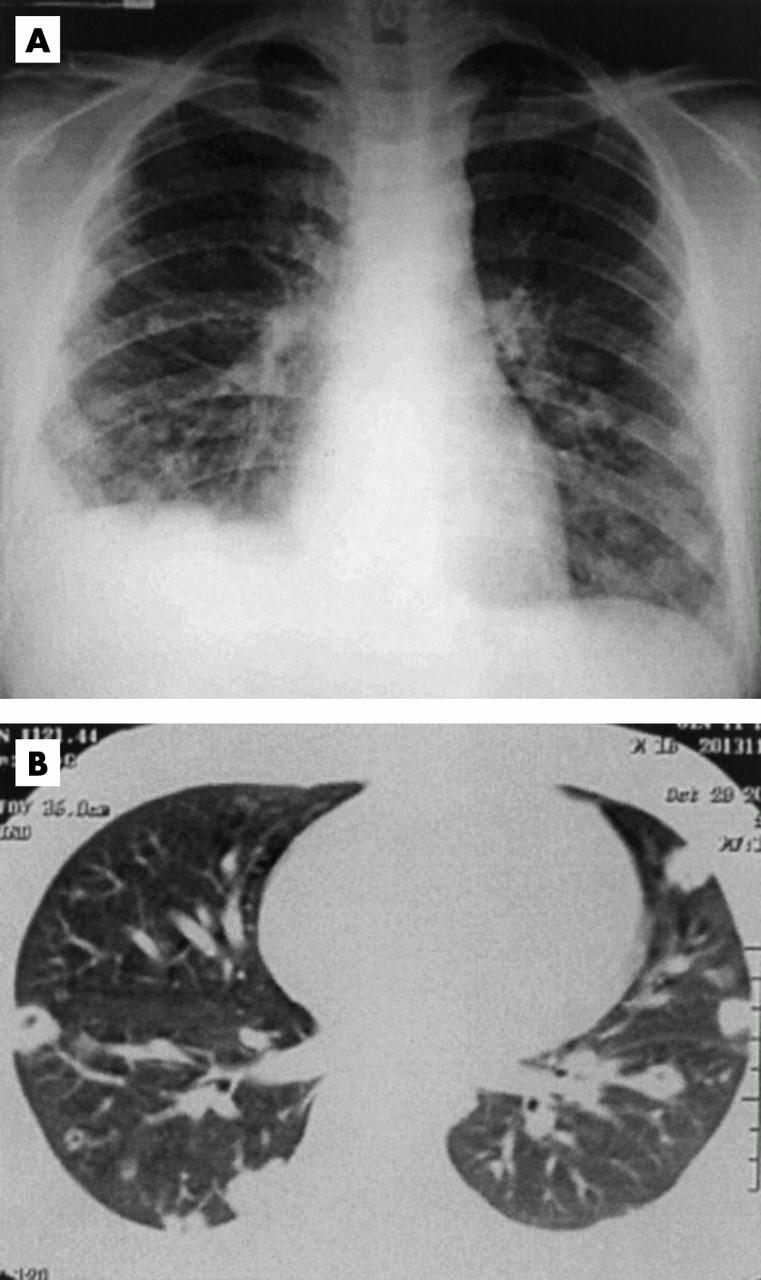
(A) Posteroanterior chest radiograph shows ill defined areas of consolidation in peripheral portions of both lower lobes (case 1). (B) CT section below carina. Scattered nodules in both solid and cavitations, most of which are compatible with haematogenous seeding (case 1).
Figure 2 .
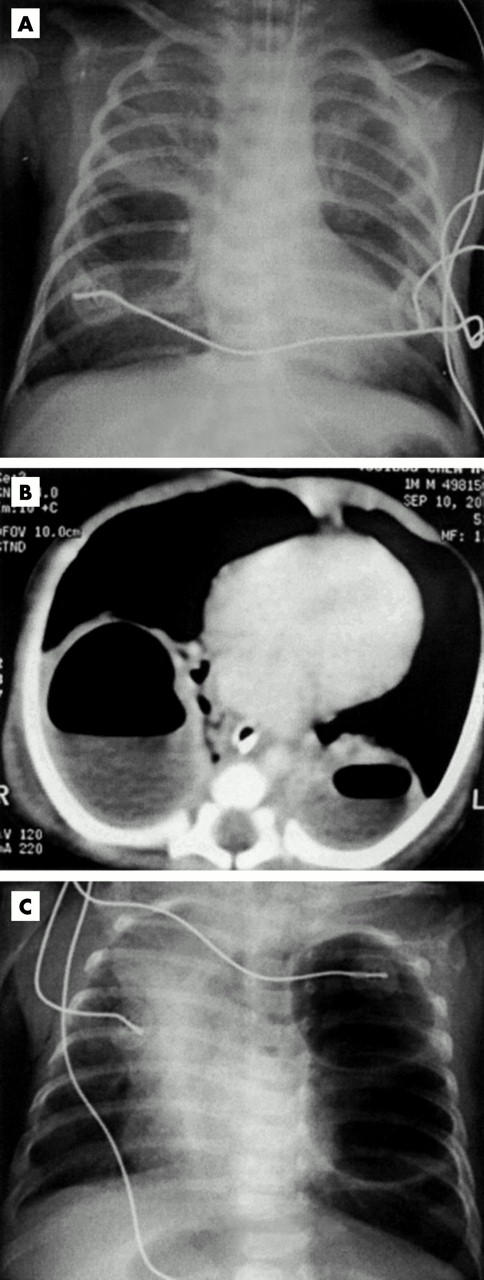
(A) Frontal chest radiograph shows large sized cavitations on both lung fields (case 10). (B) Chest CT axial view shows bilateral lung abscesses with air–fluid level (case 10). (C) Large pneumatocoele in the left lung noted two months after discharge (case 10).
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Boyce J. M. Methicillin-resistant Staphylococcus aureus. Detection, epidemiology, and control measures. Infect Dis Clin North Am. 1989 Dec;3(4):901–913. [PubMed] [Google Scholar]
- Chen M. L., Chang S. C., Pan H. J., Hsueh P. R., Yang L. S., Ho S. W., Luh K. T. Longitudinal analysis of methicillin-resistant Staphylococcus aureus isolates at a teaching hospital in Taiwan. J Formos Med Assoc. 1999 Jun;98(6):426–432. [PubMed] [Google Scholar]
- Cohen R. I., Rossoff L. J. A patient with fever and an abnormal roentgenogram. Eur Respir J. 1994 Sep;7(9):1719–1720. doi: 10.1183/09031936.94.07091719. [DOI] [PubMed] [Google Scholar]
- Coughlin W. F., Knott P. E. Right atrial myxoma. A cause of septic pulmonary emboli in an adolescent female. J Adolesc Health Care. 1990 Jul;11(4):351–354. doi: 10.1016/0197-0070(90)90047-6. [DOI] [PubMed] [Google Scholar]
- Felman A. H., Shulman S. T. Staphylococcal osteomyelitis, sepsis, and pulmonary disease. Observations of 10 patients with combined osseous and pulmonary infections. Radiology. 1975 Dec;117(3 Pt 1):649–655. doi: 10.1148/117.3.649. [DOI] [PubMed] [Google Scholar]
- Fergie J. E., Purcell K. Community-acquired methicillin-resistant Staphylococcus aureus infections in south Texas children. Pediatr Infect Dis J. 2001 Sep;20(9):860–863. doi: 10.1097/00006454-200109000-00007. [DOI] [PubMed] [Google Scholar]
- Goodwin N. J., Castronuovo J. J., Friedman E. A. Recurrent septic pulmonary embolism complicating maintenance hemodialysis. Ann Intern Med. 1969 Jul;71(1):29–38. doi: 10.7326/0003-4819-71-1-29. [DOI] [PubMed] [Google Scholar]
- Griffith G. L., Maull K. I., Sachatello C. R. Septic pulmonary embolization. Surg Gynecol Obstet. 1977 Jan;144(1):105–108. [PubMed] [Google Scholar]
- Herold B. C., Immergluck L. C., Maranan M. C., Lauderdale D. S., Gaskin R. E., Boyle-Vavra S., Leitch C. D., Daum R. S. Community-acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA. 1998 Feb 25;279(8):593–598. doi: 10.1001/jama.279.8.593. [DOI] [PubMed] [Google Scholar]
- Huang R. M., Naidich D. P., Lubat E., Schinella R., Garay S. M., McCauley D. I. Septic pulmonary emboli: CT-radiographic correlation. AJR Am J Roentgenol. 1989 Jul;153(1):41–45. doi: 10.2214/ajr.153.1.41. [DOI] [PubMed] [Google Scholar]
- Hussain F. M., Boyle-Vavra S., Bethel C. D., Daum R. S. Current trends in community-acquired methicillin-resistant Staphylococcus aureus at a tertiary care pediatric facility. Pediatr Infect Dis J. 2000 Dec;19(12):1163–1166. doi: 10.1097/00006454-200012000-00009. [DOI] [PubMed] [Google Scholar]
- Kugelman A., Weinger-Abend M., Bader D. Pulmonary cyst caused by septic emboli in the preterm infant. J Perinatol. 1998 Mar-Apr;18(2):156–159. [PubMed] [Google Scholar]
- Kuhlman J. E., Fishman E. K., Teigen C. Pulmonary septic emboli: diagnosis with CT. Radiology. 1990 Jan;174(1):211–213. doi: 10.1148/radiology.174.1.2294550. [DOI] [PubMed] [Google Scholar]
- Lautenschlager S., Herzog C., Zimmerli W. Course and outcome of bacteremia due to Staphylococcus aureus: evaluation of different clinical case definitions. Clin Infect Dis. 1993 Apr;16(4):567–573. doi: 10.1093/clind/16.4.567. [DOI] [PubMed] [Google Scholar]
- Lowy F. D. Staphylococcus aureus infections. N Engl J Med. 1998 Aug 20;339(8):520–532. doi: 10.1056/NEJM199808203390806. [DOI] [PubMed] [Google Scholar]
- MacMillan J. C., Milstein S. H., Samson P. C. Clinical spectrum of septic pulmonary embolism and infarction. J Thorac Cardiovasc Surg. 1978 May;75(5):670–679. [PubMed] [Google Scholar]
- Osei C., Berger H. W., Nicholas P. Septic pulmonary infarction: clinical and radiographic manifestations in 11 patients. Mt Sinai J Med. 1979 Mar-Apr;46(2):145–148. [PubMed] [Google Scholar]
- Rockoff M. A., Gang D. L., Vacanti J. P. Fatal pulmonary embolism following removal of a central venous catheter. J Pediatr Surg. 1984 Jun;19(3):307–309. doi: 10.1016/s0022-3468(84)80194-3. [DOI] [PubMed] [Google Scholar]
- Rossi S. E., Goodman P. C., Franquet T. Nonthrombotic pulmonary emboli. AJR Am J Roentgenol. 2000 Jun;174(6):1499–1508. doi: 10.2214/ajr.174.6.1741499. [DOI] [PubMed] [Google Scholar]
- Shah P. M. Staphylococcus aureus in lower respiratory infections: clinical relevance of antimicrobial resistance. Semin Respir Infect. 2001 Sep;16(3):196–202. doi: 10.1053/srin.2001.25625. [DOI] [PubMed] [Google Scholar]
- Shulman S. T., Ayoub E. M. Severe staphylococcal sepsis in adolescents. Pediatrics. 1976 Jul;58(1):59–66. [PubMed] [Google Scholar]
- Stine K. C., Friedman H. S., Kurtzberg J., Filston H. C., Baker M. E., Lowe J., Falletta J. M. Pulmonary septic emboli mimicking metastatic rhabdomyosarcoma. J Pediatr Surg. 1989 May;24(5):491–493. doi: 10.1016/s0022-3468(89)80410-5. [DOI] [PubMed] [Google Scholar]
- Stine K. C., Friedman H. S., Kurtzberg J., Filston H. C., Baker M. E., Lowe J., Falletta J. M. Pulmonary septic emboli mimicking metastatic rhabdomyosarcoma. J Pediatr Surg. 1989 May;24(5):491–493. doi: 10.1016/s0022-3468(89)80410-5. [DOI] [PubMed] [Google Scholar]
- Thompson R. L., Cabezudo I., Wenzel R. P. Epidemiology of nosocomial infections caused by methicillin-resistant Staphylococcus aureus. Ann Intern Med. 1982 Sep;97(3):309–317. doi: 10.7326/0003-4819-97-3-309. [DOI] [PubMed] [Google Scholar]
- Willcox P. A., Rayner B. L., Whitelaw D. A. Community-acquired Staphylococcus aureus bacteraemia in patients who do not abuse intravenous drugs. QJM. 1998 Jan;91(1):41–47. doi: 10.1093/qjmed/91.1.41. [DOI] [PubMed] [Google Scholar]
- Yao T. C., Hung I. J., Su L. H., Chiu C. H. Endogenous endophthalmitis and necrotising pneumonia caused by Klebsiella pneumoniae in a child with beta-thalassaemia major. Eur J Pediatr. 2001 Jul;160(7):449–449. doi: 10.1007/s004310100764. [DOI] [PubMed] [Google Scholar]