

Abstract
Atrioventricular conduction disease may occur in a range of conditions. If echocardiography suggests the presence of an infiltrative cardiomyopathy the diagnosis of amyloidosis may be confirmed by subcutaneous fat sampling from the site of pacemaker implantation. This technique requires no additional invasive procedure and confers no extra risk for the patient. Confirmation of amyloidosis provides important prognostic information and may allow specific treatment.
Keywords: amyloidosis, fat sampling
A 71 year old British white man was referred to a cardiothoracic centre for permanent cardiac pacing. He had presented with an 18 month history of exertional dyspnoea and an episode of syncope. Chest radiography had shown cardiomegaly and pulmonary oedema for which he had received diuretics and angiotensin converting enzyme inhibitors with some symptomatic relief. An ECG showed first degree heart block, left axis deviation, and right bundle branch block—that is, trifascicular block. An echocardiogram showed severe asymmetrical thickening of the left ventricular wall, with a septum 2 cm thick (normal < 1.1 cm) but normal internal dimensions. The left atrium was mildly dilated. The valve structures were normal and there was a small pericardial effusion. The right ventricular free wall was also diffusely thickened (fig 1).
Figure 1.
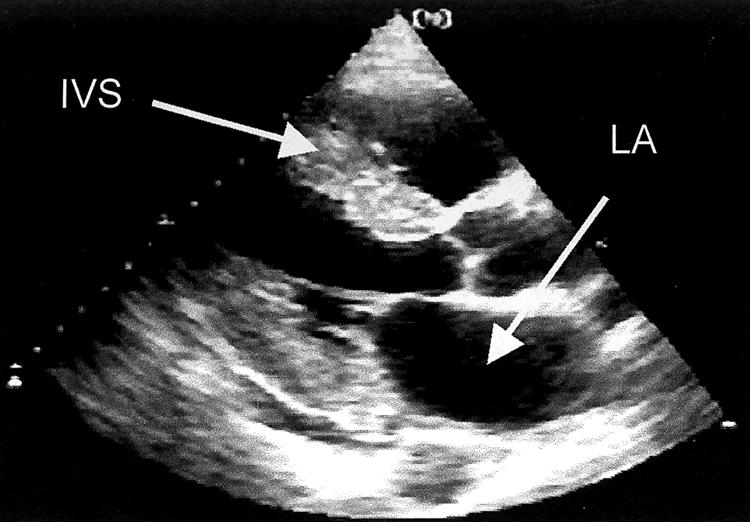
Transthoracic parasternal long axis echocardiogram. IVS, interventricular septum; LA, left atrium.
During the insertion of a dual chamber pacemaker, a sample of subcutaneous fat was taken from the prepectoral tissues and sent for histological examination. Areas of amorphous material stained with Congo red produced apple green birefringence under cross-polarised polarised light, confirming a diagnosis of amyloidosis. Subsequent immunohistochemical staining with antibodies to transthyretin showed that the amyloid deposits were of transthyretin type (fig 2). DNA sequencing showed that the patient was heterozygous for the known amyloidogenic variant transthyretin alanine 60, which is most often identified in those of Irish ancestry.
Figure 2.
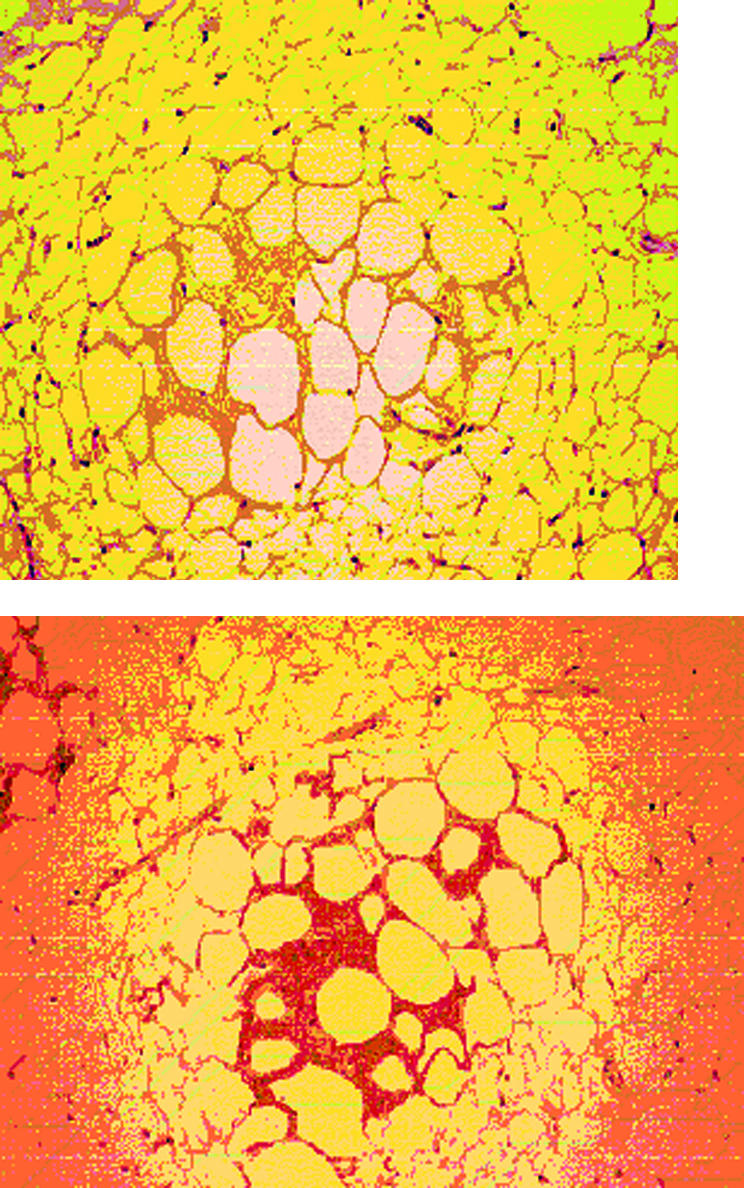
Fat biopsy, stained with Congo red (upper panel), showing amyloid deposits that stained immunohistochemically with antibodies to transthyretin type (lower panel).
DISCUSSION
Cardiac amyloidosis can present with symptoms of left or right ventricular dysfunction, orthostatic hypotension, or conduction disease. The diagnosis is strongly supported by echocardiography that shows increased thickness of ventricular walls, sometimes with a granular appearance, atrial enlargement, thickened valves, and diastolic dysfunction, especially in a patient with no history of hypertension. Systolic impairment is a late feature.
Cardiac amyloid is always a manifestation of systemic amyloidosis, although the significance and prognosis depend greatly on the amyloid fibril type. Monoclonal immunoglobulin light chain amyloidosis is the most serious and frequently diagnosed form of cardiac amyloid, but cardiac amyloid derived from wild-type transthyretin, which often causes no symptoms, occurs in about one quarter of very elderly people. Cardiac transthyretin amyloid in younger people is frequently associated with a mutation in the transthyretin gene, as described here. Indeed, 4% of African Americans are heterozygous for the amyloidogenic transthyretin variant isoleucine 122.1
Diagnosis of amyloidosis generally requires histological confirmation. Biopsy also allows immunohistochemical analysis of the amyloid fibril type. In the case of hereditary transthyretin amyloidosis this has implications for genetic counselling and in younger patients may be an indication for liver transplantation, which ameliorates the underlying metabolic abnormality. Target organ biopsies, for example from the endomyocardium, are usually diagnostic but are invasive and not without risk.2,3 Biopsies from accessible sites such as the rectum and abdominal fat are safer to obtain and frequently diagnostic.4
Samples of fat have considerable diagnostic potential in amyloidosis and may be obtained during a variety of procedures. This case illustrates the value of fat sampling during pacemaker implantation when cardiac amyloidosis is suspected and pacemaker implantation is required. It also highlights the occasional hereditary aetiology of cardiac amyloidosis and the vital roles of immunohistochemistry and DNA analysis in its evaluation.
REFERENCES
- 1.Jacobson D, Pastore R, Yaghoubian R, et al. Variant-sequence transthyretin (isoleucine 122) in late-onset cardiac amyloidosis in black Americans. N Engl J Med 1997;336:466–73. [DOI] [PubMed] [Google Scholar]
- 2.Baraldi-Junkins C, Levin H, Kasper E, et al. Complications of endomyocardial biopsy in heart transplant patients. J Heart Lung Transplant 1993;12:63–7. [PubMed] [Google Scholar]
- 3.Quinton Gradeck W, D'Amico C, Smith A, et al. Routine surveillance endomyocardial biopsy continues to detect significant rejection late after heart transplantation. J Heart Lung Transplant 2001;20:497–502. [DOI] [PubMed] [Google Scholar]
- 4.Spyrou N, Foale R. Restrictive cardiomyopathies. Curr Opin Cardiol 1994;9:344. [DOI] [PubMed] [Google Scholar]