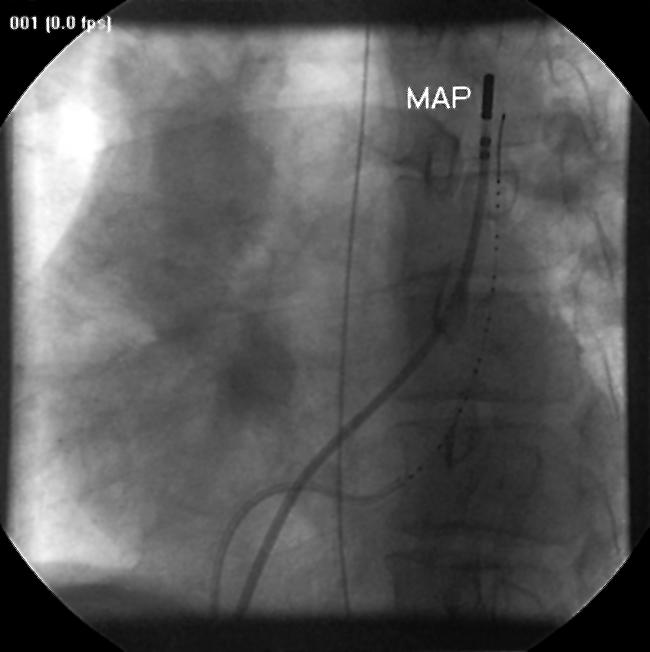
A 33 year old man was referred to our centre for radiofrequency catheter ablation for clinically documented atrial flutter. A persistent left superior vena cava (PLSVC) draining into a dilated coronary sinus was revealed during angiography. During tachycardia and thereafter in sinus rhythm, endocardial mapping of the right atrium and the PLSVC was performed by using electroanatomic mapping (CARTO, Biosense Webster Ltd, Tirat-HaCarmel, Israel). An isthmus dependent counterclockwise atrial flutter was defined as the mechanism of the tachycardia which was successfully ablated by radiofrequency ablation. Rapid spread of activation (speed 1.66 m/s) from right atrium to PLSVC during tachycardia was demonstrated in the activation map (below, left panel; LAO view; SVC, superior vena cava; RA, right atrium; TA, tricuspid annulus; CS, coronary sinus). Bipolar voltage map (right panel) showed distribution of potentials throughout the aberrant vein with the highest value of 6.05 mV recorded in the mid sections of the structure. Pacing from multiple sites within PLSVC, even from positions beyond the cardiac silhouette (white points on both electroanatomic maps) captured the structure and activation propagated through the atria. LAO fluoroscopic view showed the highest site within PLSVC where capture could be achieved by pacing from mapping catheter (below right, MAP, mapping catheter).
This presentation demonstrates the existence of muscle fibres surrounding the PLSVC and highlights the possibility that the presence of surrounding muscle sleeves could be a general feature of most of the veins that enter the cardiac chambers.
Figure 1.

Figure 2.