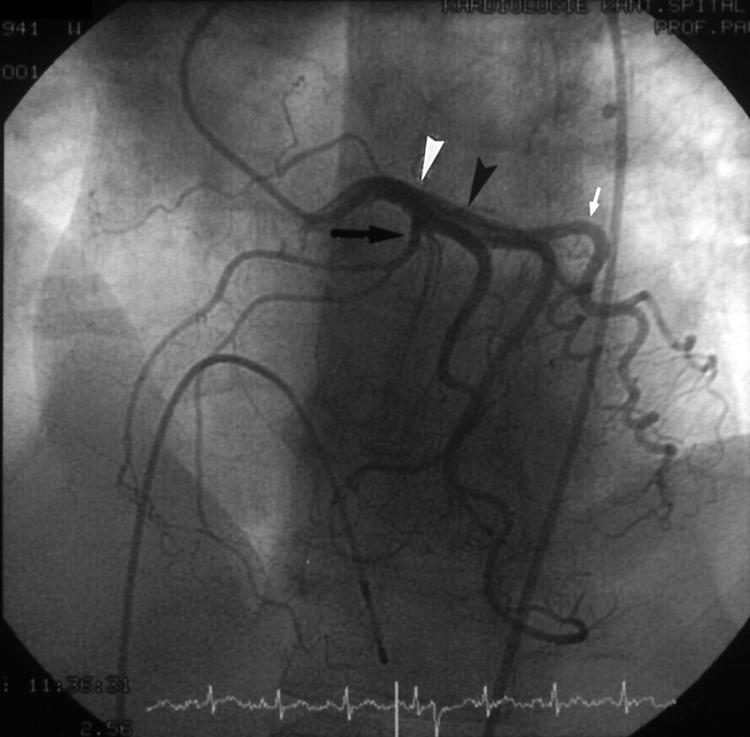
A 60 year old women presented with chest pain to our department. Risk factors for coronary artery disease included hypertension and hypercholesterolaemia. Her coronary angiogram (see panels) showed normal left anterior descending (LAD) and circumflex (CXF) coronary arteries. However, the right coronary artery (RCA) originated from the mid LAD (RCA, wide black arrow; LAD, white arrowhead; first diagonal, black arrowhead; CXF, white narrow arrow). No collateral circulation from the left to the right coronary artery was observed. There was no evidence of external compression of the proximal portion of the RCA during systole or diastole. Acetylcholine infusion did not cause vasoconstriction of the coronary artery. On the basis of these results we felt there was no evidence of coronary artery disease or vasospastic angina.
Coronary artery anomalies are present in 1–2% of the population who undergo coronary angiography. Single coronary arteries are very rare, with a necropsy incidence of 0.29%. RCA originating from the left main coronary artery accounts for only 0.65% of these anomalies.
Figure 1.
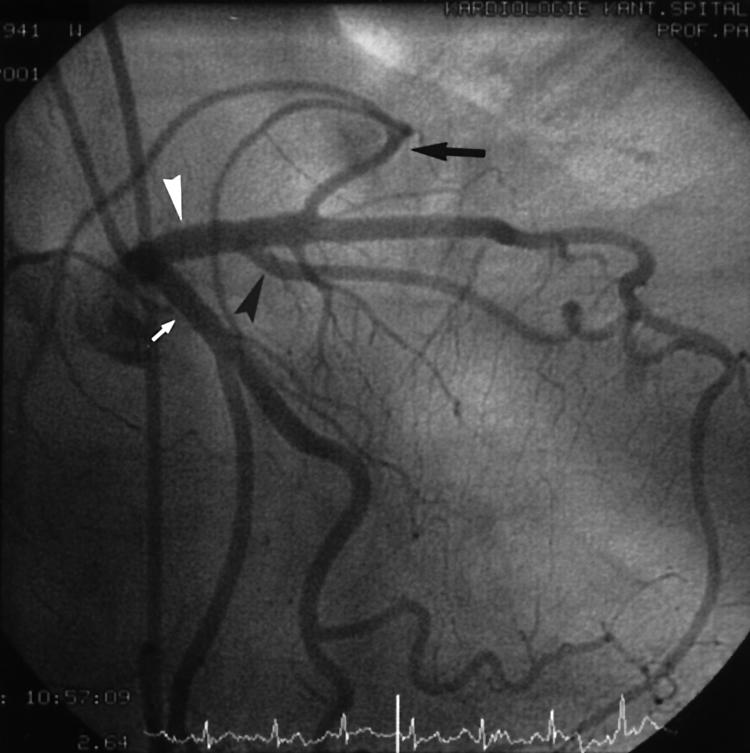
Figure 2.