

Abstract
Brachytherapy is a proposed treatment for in-stent restenosis and is the subject of several clinical trials and debates. The standard treatment of patients with variant angina is to eliminate vasoconstrictive factors and to administer vasodilating drugs. This is the first description of successful brachytherapy for coronary spasm.
Keywords: brachytherapy, restenosis, angina, coronary spasm
A 48 year old man was admitted to hospital for unstable angina lasting one week. He had a history of inferior myocardial infarction with acute percutaneous coronary intervention of the right coronary artery six years previously and percutaneous coronary intervention of the circumflex artery two years previously. Radiation therapy (brachytherapy) of the circumflex artery for restenosis had been carried out two months previously. Cardiac risk factors were hypertension, hypercholesterolaemia, family history, and tobacco use. His medication comprised aspirin, clopidogrel, amlodipine, and nebivolol. Cardiac catheterisation showed arteriosclerotic plaques without significant stenosis of the coronary arteries. An acetylcholine test (intracoronary infusions of acetylcholine) showed pronounced coronary spasm of the right and left coronary arteries (fig 1). The coronary flow reserve was normal. Nicorandil was added to the patient’s medication regimen. However, despite the extensive pharmacological treatment the patient continued to complain of daily angina at rest. We decided to apply 20 Gy on the right coronary artery vessel wall through a β emitting wire source centred by a Galileo balloon (Guidant Corp, Indianapolis, Indiana, USA). After two months the acetylcholine test was repeated and in the radiated portion of the right coronary artery no more coronary spasms were documented (fig 2). Therefore, brachytherapy was extended to the left anterior descending artery. The patient was free of complaints following the brachytherapy.
Figure 1.
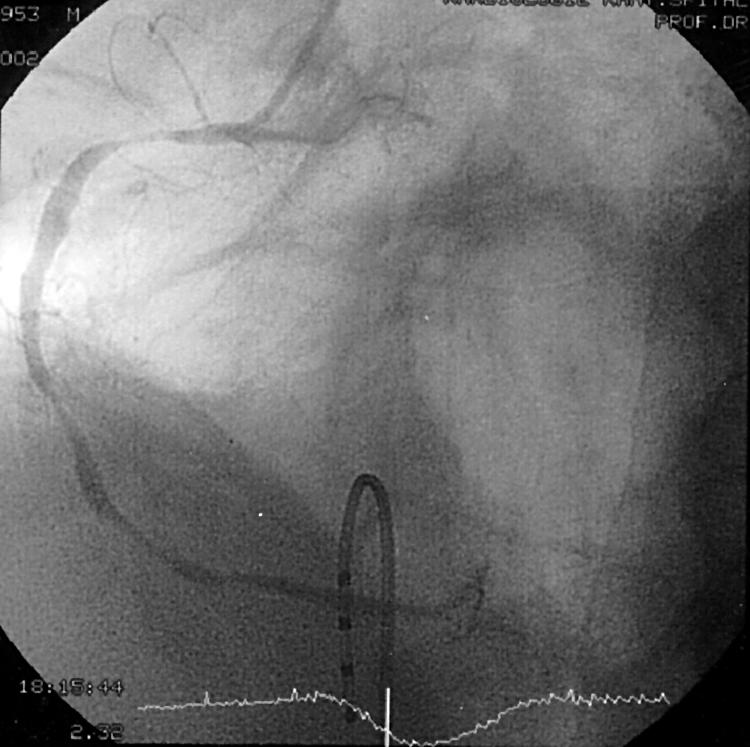
Coronary angiography of the right coronary artery (RCA) after intracoronary injection of acetylcholine. The angiography shows diffuse coronary spasm of the RCA.
Figure 2.
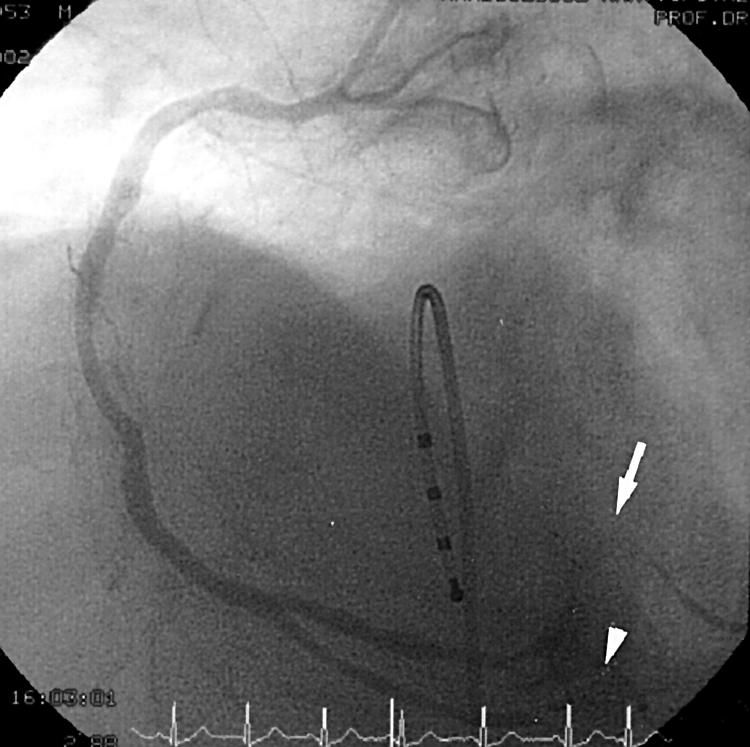
Coronary angiography of the RCA two months after brachytherapy of the RCA, including proximal ramus posterolateralis dexter and proximal ramus interventricularis posterior, after intracoronary injection of acetylcholine. Coronary spasm is evident in the distal ramus interventricularis posterior (arrowhead) and distal part of ramus posterolateralis dexter (arrow). In this portion of the RCA no radiation was applied by a β emitting source.
DISCUSSION
Variant angina was described in 1959 by Prinzmetal and colleagues1 and later recognised as a consequence of coronary spasm in normal coronary arteries.2 Coronary spasm is a multifactorial process (endothelial dysfunction, hypersensitivity to vasoconstrictor stimuli, hypercontractility of vascular smooth muscle). Coronary artery spasm may also have a broader role in patients with arteriosclerotic coronary artery disease.3 Intracoronary infusion of acetylcholine has been shown to induce severe coronary spasm in patients with variant angina.4 The standard treatment of patients with variant angina is to eliminate vasoconstrictive factors (cigarette smoking, hyperventilation, and cocaine use) and administer vasodilating drugs. Despite extensive treatment with vasodilators (nitrates, calcium antagonist, nicorandil, and nebivolol), our patient complained of daily angina and thus we sought an alternative mode of clinical management.
Brachytherapy is a recently proposed treatment for in-stent restenosis and is the subject of a clinical trials and debate.5,6 The first clinical trial of treatment with γ radiation was initiated in 1990 in patients with in-stent restenosis of femoropopliteal arteries.7 Brachytherapy of human coronary arteries was first performed by Condado and colleagues in 1995.8 In 1997, Teirstein showed the effectiveness of brachytherapy for treatment of in-stent restenosis.9 The cause of restenosis is lumen loss after percutaneous coronary intervention by neointimal growth and vessel shrinkage. The effectiveness of brachytherapy in the treatment of restenosis is a result of selective inactivation of smooth muscle cells and myofibroblasts and, at a high radiation dose, to complete elimination of their proliferative capacity.10 Elimination of vasospasm after brachytherapy is also probably due to destruction of the endothelium and smooth muscle cells. To our knowledge this is the first described case of brachytherapy for coronary spasm.
REFERENCES
- 1.Prinzmetal M, Kennamer R, Merliss R. A variant form of angina pectoris. Am J Med 1959;27:375. [DOI] [PubMed] [Google Scholar]
- 2.Cohen M. Variant angina pectoris. In: Fuster V, Ross R, Topo JB. Cardiovascular thrombosis. Philadelphia: Lippincott, 1996:1367–76.
- 3.Conti CR. Myocardial infarction: thoughts about pathogenesis and the role of coronary artery spasm. Am Heart J 1985;110:185. [DOI] [PubMed] [Google Scholar]
- 4.Ludmer PL, Selwyn AP, Shook TL, et al. Paradoxical vasoconstriction induced by acetylcholine in atherosclerotic coronary arteries. N Engl J Med 1986;315:1046–51. [DOI] [PubMed] [Google Scholar]
- 5.Kuntz RE, Baim DS. Prevention of coronary restenosis: the evolving evidence base for radiation therapy. Circulation 2000;101:2130–3. [DOI] [PubMed] [Google Scholar]
- 6.Sheppard R, Eisenberg MJ. Intracoronary radiotherapy for restenosis. N Engl J Med 2001;344:295–7. [DOI] [PubMed] [Google Scholar]
- 7.Liermann D, Bottcher HD, Kolath J, et al. Prophylactic endovascular radiotherapy to prevent intimal hyperplasia after stent implantation in femoropopliteal arteries. Cardiovasc Intervent Radiol 1994;17:12–6. [PubMed] [Google Scholar]
- 8.Condado JA, Waksman R, Gurdiel O, et al. Long-term angiographic and clinical outcome after percutaneous transluminal coronary angioplasty and intracoronary radiation in humans. Circulation 1997;96:727–32. [DOI] [PubMed] [Google Scholar]
- 9.Teirstein PS, Massullo V, Jani S, et al. Catheter-based radiotherapy to inhibit restenosis after coronary stenting. N Engl J Med 1997;336:1697–703. [DOI] [PubMed] [Google Scholar]
- 10.Fareh J, Martel R, Kemani P, et al. Cellular effects of betaparticle delivery on vascular smooth muscle cells and endothelial cells. a dose-response study. Circulation 1999;99:1477–84. [DOI] [PubMed] [Google Scholar]