

Abstract
Computed tomographic virtual cardioscopy was used to provide clear and precise visualisation of a myxoma with a stalk arising from the interatrial septum. This technique permits the safe, reliable, and non-invasive diagnosis of intracardiac lesions. This case is presented to assist the cardiovascular surgeon in preoperative planning or in developing a simulation of robotic cardiac surgery.
Keywords: computed tomographic cardioscopy, virtual cardioscopy, atrial myxoma, simulator, robotic cardiac surgery
A 59 year old women presented with exertional dyspnoea, orthopnoea, decreased urine output, and lower leg oedema for the month preceding her admission. During examination in our outpatient department, a grade II/VI pansystolic murmur was noted. After admission, plain chest radiography showed mild cardiomegaly with punctate calcifications superimposed at the location of the left atrium (fig 1). Echocardiograms showed a left atrial tumour with severe mitral regurgitation. To determine the nature of this tumour, cardiac electron beam computed tomography (CT) (C-150L, Imatron, South San Francisco, California, USA) was performed. The scans showed a large low attenuating (similar to subcutaneous fat) mass with a stalk attached to the interatrial septum and calcified spots on its margins in the left atrium (fig 2). Three dimensional reconstructed images with a virtual reality effect were created on a work station (SUN Sparc 10, Sun Microsystems, Mountain View, California, USA). Through the foggy appearance of the cardiac chambers, the global appearances of the left atrial tumour could be directly visualised, as with real endoscopy. This tumour had a stalk arising from the interatrial septum (fig 2A) and it occupied nearly half the area of the mitral annulus (dotted line in fig 2B). The angiocardiographic and surgical findings subsequently confirmed the anatomy. Results of pathological analysis also confirmed that this lesion was a myxoma.
Figure 1.

Lateral chest radiograph showing mild cardiomegaly, with punctate calcifications superimposed at the location of the left atrium.
Figure 2.
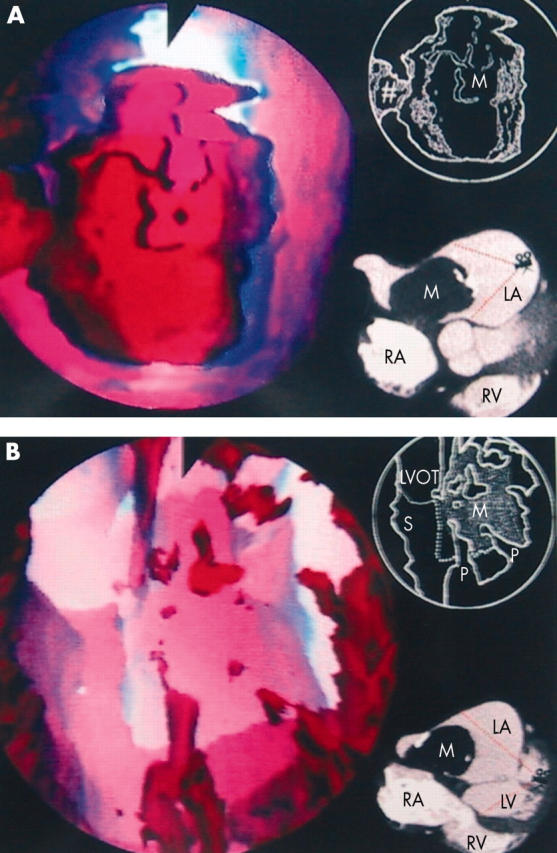
(A) Virtual cardioscopic view from the left lateral aspect of the left atrium (LA) towards the right atrium (RA). The tumour had a stalk (#), which arose from the interatrial septum (S). (B) Virtual cardioscopic view from left ventricular apex towards the left ventricular outflow tract (LVOT) and mitral annulus. The tumour occupied nearly half the area of the mitral opening. The corresponding diagrams and electron beam computed tomographic sections are shown in the right upper and lower corners, respectively. LV, left ventricle; M, myxoma; RV, right ventricle; P, papillary muscle.
DISCUSSION
CT virtual colonoscopy is a safe, non-invasive technique for evaluating the entire surface of the colon and for detecting polyps or cancers. This technique has excellent sensitivity and specificity for the detection of colorectal neoplasms 10 mm or larger.1 The virtual endoscopic simulator can identify differences between beginners and experts in gastrointestinal endoscopy. A three week training period has been shown to improve significantly the performance of beginners.2 Nowadays, more and more papers are discussing video assisted cardioscopy3 and robotic techniques4 for intracardiac surgery. However, the heart rate is faster than the rate of colon peristalsis, and the result is additional motion artefact with conventional CT (scanning time for one section is 600–1000 ms), which uses a standard x ray tube. Because of the short scanning time for electron beam CT (scanning time for one section is 100 ms), electrocardiographic gating may enable clear imaging of the demarcations of the intracardiac lesion without motion artefacts.5 With the help of the three dimensional reconstruction plus a virtual reality technique, CT virtual cardioscopic images could be created, similar to real endoscopic images. To our knowledge, this capability has never been reported in the literature. These pictures allow direct observation of the pathology and anatomy within the heart, and the findings can subsequently be confirmed by the angiocardiographic and surgical results.
A comparison of the diagnostic yields with echocardiography, catheterisation, and CT virtual cardioscopy shows that CT virtual cardioscopy is superior to echocardiography and catheterisation in visualising the intracardiac anatomy in any plane. In addition, the source CT images are inspected first to clearly detect associated visceral, bronchopulmonary, mediastinal, and intracardiac anomalies at the same time,5 as these findings can affect the surgical intervention. With this procedure, surgeons can anticipate difficulties in using video assisted surgical techniques or robotic cardiac surgery, and they can develop a simulator for beginners to improve their performance.
This technique permits the safe, reliable, and non-invasive diagnosis of intracardiac lesions. We believe that it has the potential for wider applicability in providing a preview of real cardioscopy. This information will assist the cardiovascular surgeon in preoperative planning or in developing a simulator of robotic cardiac surgery.
REFERENCES
- 1.Macari M, Bini EJ, Xue X. Colorectal neoplasms: prospective comparison of thin-section low-dose multi-detector row CT colonography and conventional colonoscopy for detection. Radiology 2002;224:383–92. [DOI] [PubMed] [Google Scholar]
- 2.Ferlitsch A, Glauninger P, Gupper A, et al. Evaluation of a virtual endoscopy simulator for training in gastrointestinal endoscopy. Endoscopy 2002;34:698–702. [DOI] [PubMed] [Google Scholar]
- 3.Miyaji K, Murakami A, Suematsu Y, et al. Video-assisted cardioscopy for infectious endocarditis. Pediatr Cardiol 2002;23:562–3. [DOI] [PubMed] [Google Scholar]
- 4.Nifong LW, Chu VF, Bailey BM, et al. Robotic mitral valve repair: experience with the da Vinci system. Ann Thorac Surg 2003;75:438–42 discussion 443. [DOI] [PubMed] [Google Scholar]
- 5.Chen SJ, Li YW, Wang JK, et al. Usefulness of electron beam computed tomography in children with heterotaxy syndrome. Am J Cardiol 1998;81:188–94. [DOI] [PubMed] [Google Scholar]