A 56 year old woman presented for elective percutaneous coronary intervention (PCI), following the recurrence of limiting angina two years after coronary bypass operation. In this short time, the saphenous vein graft to her right coronary artery had blocked, and the left internal mammary artery (LIMA) anastomosed to her left anterior descending artery (LAD) showed a long, severe, heavily calcified stenosis proximal to the anastomosis. As the native vessels were not amenable to PCI, a decision was made to tackle the LIMA-LAD lesion.
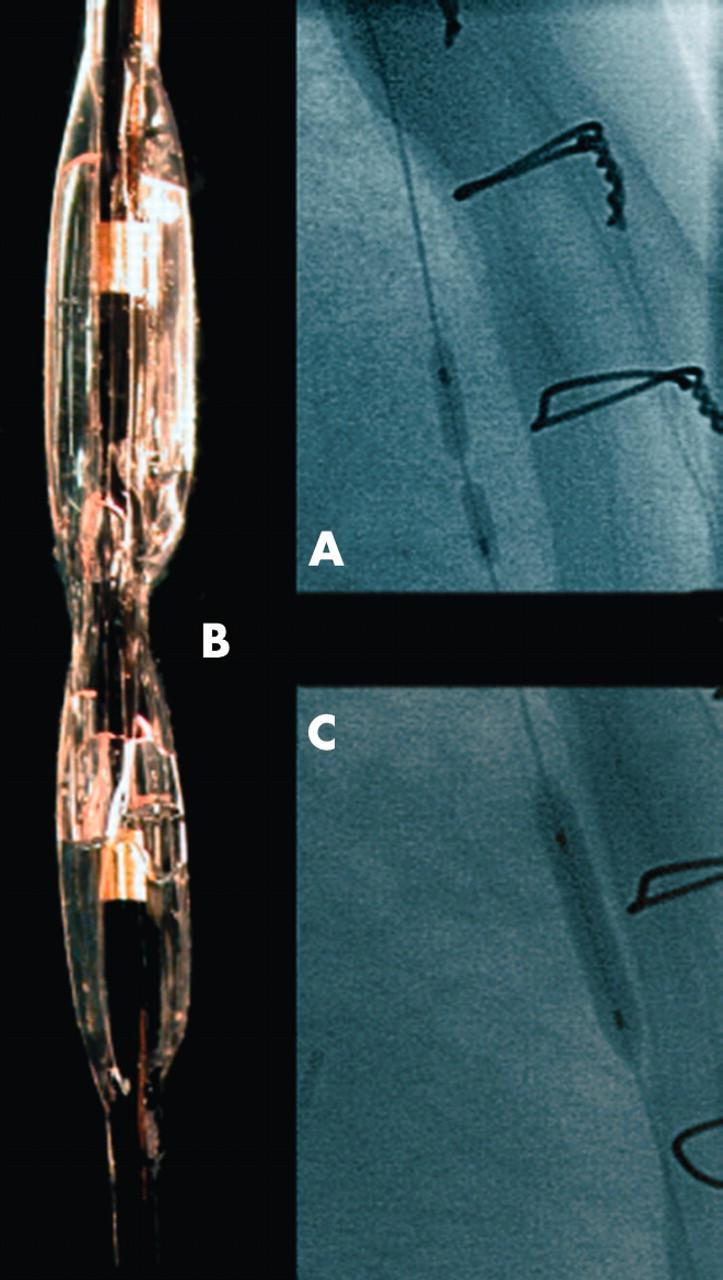
The lesion was crossed with a BMW guidewire and balloon pre-dilatation attempted. However, multiple coronary balloons (diameters 2.0–3.0 mm) failed to crack the severely calcified stenosis (panel A) Two balloons ruptured (inflation pressures being more than 20 atm), leading to localised coronary dissection. Usage of cutting balloon (Boston Scientific), which includes microsurgical blades to incise the calcified plaque, was attempted, but even high inflation pressures failed to impact on the narrowing. One of the ruptured balloons (Boston Scientific Maverick 2.0 mm balloon, inflated at 22 atm), retained the circumferential shape of the stenosis even after removal and washing (panel B). Eventually, an oversized 3.5 semi-compliant balloon (Medtronic Extensor 3.5 mm) succeeded in dilating the stenosis (panel C), that was then successfully treated with a drug eluting stent.
The treatment of non-dilatable, severely calcified stenosis remains challenging. The use of rotational ablation techniques (for example, Rotablator) may solve the problem, but vessel tortuosity may limit their utility in distally located stenoses. In this setting, using an oversized semi-compliant or a non-compliant balloon, with careful step-by-step inflations, may be helpful by permitting an increase of radial dilation force.
Figure 1.