

Abstract
This report hypothesises an active role for the acute phase protein, C reactive protein (CRP), in local inflammatory reactions. This was studied in infarction sites from liver and kidney in a patient who died as a result of multiple complications after cholecystectomy. In this patient, a general acute phase protein reaction was induced, with an increase in plasma CRP. In infarction sites of kidney and liver, colocalisation of CRP and activated complement were found, whereas non-infarct sites were negative for CRP and complement. These results suggest that CRP directly participates in local inflammatory processes, possibly via complement activation, after binding of a suitable ligand.
Keywords: C reactive protein, infarcted tissue, sepsis, complement
The physiological role of the acute phase protein C reactive protein (CRP) is not fully understood. It has been suggested that circulating CRP only reflects the extent of the acute phase reaction in response to non-specific stimuli. In contrast, studies have shown CRP to be localised in inflamed tissues (synovium and brain),1,2 and in atherosclerotic vessels or inflamed myocardium.3,4 Furthermore, recently for the first time we have found the formation of CRP–complement complexes in infarcted myocardial tissue (R Nijmeijer et al, 2001, unpublished results). We hypothesise that CRP plays an active role in local inflammatory reactions, and that in vitro CRP activates complement after binding to a suitable ligand.5
“We hypothesise that C reactive protein plays an active role in local inflammatory reactions, and that in vitro C reactive protein activates complement after binding to a suitable ligand”
Our study on a patient who died of multiple complications after cholecystectomy, strengthens the specific role of CRP in local inflammation. This patient, a 46 year old woman, suffered from hypovolaemic shock after cholecystectomy, six weeks before death. Thereafter, she developed necrosis of the intestine (12 days before death) and multiple areas of infarction in kidneys and liver (six days before death). Furthermore, she developed sepsis (14 days before death), and the last measured CRP value was 149 mg/litre (normal value, 0–7) three days before death. To study the role of CRP, we performed immunohistochemical staining of the liver and kidney. Permission to use left over material (including fetal material) after the usual diagnostic process has been completed is part of the standard patient contract in our hospital.
In kidney and liver, CRP depositions were found in the infarcted tissue sites, with colocalisation of activated complement (fig 1A,B). In the liver, jeopardised hepatocytes and bile canaliculi stained for CRP. In the kidneys, CRP was found in jeopardised tubules and partly in glomeruli. In contrast, the non-infarcted sites did not stain for CRP. Moreover, liver and kidney tissues from an immature spontaneously aborted fetus, which can be regarded as non-ischaemic tissue controls,4 did not stain for CRP or complement either.
Figure 1.
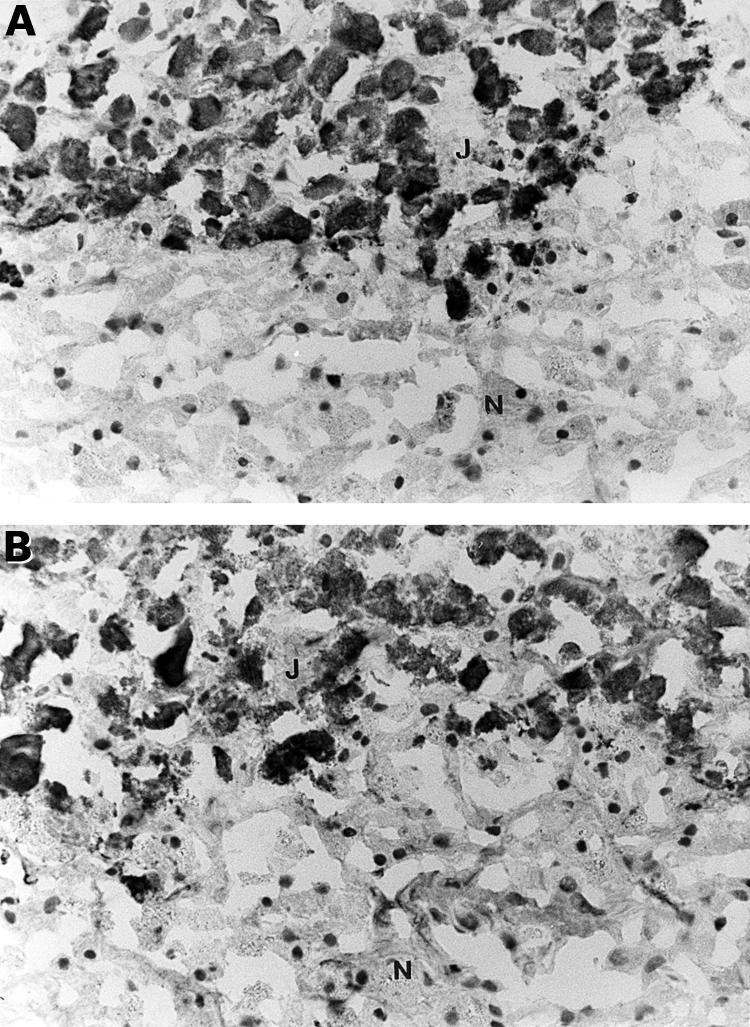
Immunohistochemical staining of (A) C reactive protein (monoclonal antibody 564; 1/500 dilution) and (B) complement (monoclonal antibody C3–15; 1/1000 dilution) in infarcted liver (J, jeopardised; N, normal). Original magnification, ×100.
Furthermore, staining for CRP was not found in the liver or kidney tissue from an adult patient who died after cerebrovascular accident (which resulted in an increased CRP value in the blood). Therefore, depositions of CRP and complement in infarcted areas are not caused by non-specific binding after death. However, we cannot definitely exclude the possibility that other substances able to activate complement are also generated in the infarcted tissue.
In the heart, complete lactate dehydrogenase decolouration of the entire left ventricle was found, without microscopical signs of infarction (including electron microscopy), suggesting terminal ischaemia. Immunohistochemical staining of the heart for CRP and activated complement was negative. This is in agreement with our findings that depositions of CRP can be found only in infarction sites in the heart beyond 12 hours.4
In conclusion, in this patient with sepsis, resulting in an increase in plasma CRP, CRP and complement were localised specifically to infarcted tissue (kidney and liver), underlining the hypothesis that CRP directly participates in local inflammatory and necrotising processes, possibly via complement activation, after binding of a suitable ligand.
Take home messages.
In this patient with sepsis, C reactive protein (CRP) and complement were localised specifically to infarcted tissue (kidney and liver)
This supports the hypothesis that CRP directly participates in local inflammatory and necrotising processes, possibly via complement activation, after binding of a suitable ligand
Acknowledgments
This study was financially supported by the Netherlands Heart Foundation, grant 93–119; 97–088. Dr Niessen is a recipient of the Dr E Dekker programme of the Netherlands Heart Foundation (D99025).
Abbreviations
CRP, C reactive protein
REFERENCES
- 1.Gitlin JD, Gitlin JI, Gitlin D. Localizing of C-reactive protein in synovium of patients with rheumatoid arthirtis. Arthritis Rheum 1977;20:1491–9. [DOI] [PubMed] [Google Scholar]
- 2.Du Clos TW, Mold C, Paterson PY, et al. Localization of C-reactive protein in inflammatory lesions of experimental allergic encephalomyelitis. Clin Exp Immunol 1981;43:565–73. [PMC free article] [PubMed] [Google Scholar]
- 3.Kushner I, Rakita I, Kaplan MH. Studies of the acute phase-protein, II: Localization of Cx-protein in heart in induced myocardial infarction in rabbits. J Clin Invest 1963;42:286–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lagrand WK, Niessen HWM, Wolbink GJ, et al. C-reactive protein colocalizes with complement in human hearts during acute myocardial infarction. Circulation 1997;95:97–103. [DOI] [PubMed] [Google Scholar]
- 5.Hack CE, Wolbink GJ, Schalkwijk C, et al. A role for secretory phospholipase A2 and C-reactive protein in the removal of injured cells. Immunol Today 197;18:111–15. [DOI] [PubMed]