

When interpreting lymph node biopsies it is sometimes necessary to distinguish the different compartments of the lymph node. In normal lymph nodes the task may be easily accomplished, but it can be difficult for effaced lymph nodes. We compared the usefulness of routinely used endothelial markers for distinguishing sinuses from vascular channels in the lymph node.
Eighteen lymph nodes—seven normal lymph nodes from a patient with colonic cancer (patient 1), eight from a patient affected by diffuse large B cell lymphoma of the stomach (patient 2), and three from a patient with anaplastic large cell lymphoma (ALCL) (patient 3)—were selected from the archives of the department of pathology, Kariya General Hospital, Japan. The tissues were fixed in 10% formalin and embedded in paraffin wax. Standard tissue sections, 6 μm thick, were stained with haematoxylin and eosin. Immunohistochemical staining was performed by means of the Ventana immunostainer (Ventana, Tacson, Arizona, USA). The primary antibodies used were commercially available antibodies directed against factor VIII (prediluted; Dako, Carpenteria, California, USA), CD31 (prediluted; Dako), and CD34 (prediluted; Dako). Positive and negative controls were used in each assay. For anti-CD34, dewaxed sections were pretreated in a microwave for 15 minutes, in 95°C 10mM citrate buffer at pH 6.0. For anti-CD31, sections were pretreated in two ways, either with trypsin or by the microwave method.
Anti-CD34 was applied to the sections of all lymph nodes from patients 1 and 2, but only decorated vascular channels. For anti-factor VIII, background staining was very intense in the sinuses. Anti-CD31, when pretreated with either trypsin or in the microwave, was positive not only for the endothelium of vascular channels but also for the lining cells of sinuses. When applied to the lymph nodes from patient 3, all the tumour cells were confined within spaces that were lined by CD31 positive cells (fig 1). The application of anti-CD34 suggested that these spaces were in fact sinuses (fig 2), leading to the conclusion that this case represented ALCL with a sinus pattern of involvement.
Figure 1.
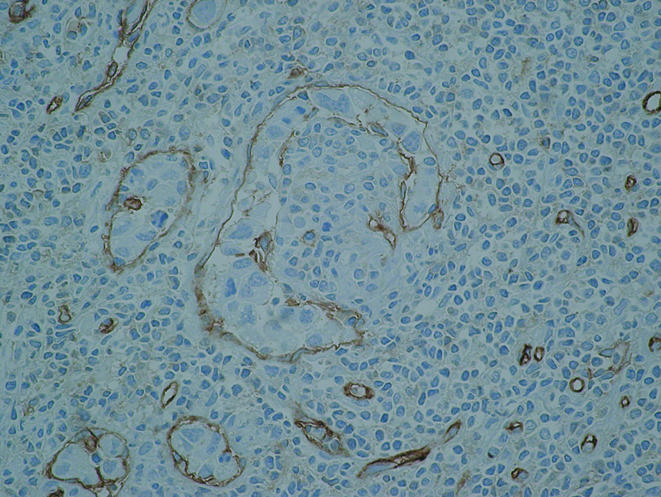
Applied to an anaplastic large cell lymphoma (ALCL) case, CD31 decorates both vascular channels and sinuses that are filled with ALCL cells (diaminobenzidine reaction; haematoxylin counterstain; original magnification, ×100).
Figure 2.
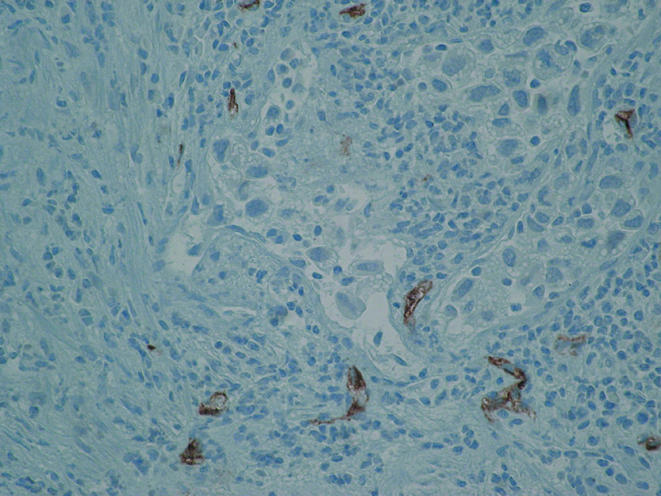
Staining for CD34 verifies that these channels are in fact sinuses (diaminobenzidine reaction; haematoxylin counterstain; original magnification, ×100).
The sinuses of the lymph node are different from vascular channels in that they are not lined with endothelium.1 CD31 is believed to be a highly specific marker for endothelial cells.2 Recently, however, McKenney and associates showed that the expression of CD31 by macrophages could easily be detected on formalin fixed, paraffin wax embedded sections, causing misdiagnosis in surgical pathology practice.3 This characteristic of CD31 may also be important in distinguishing the compartments of the lymph node or spleen. The presence of CD31 cannot be used to distinguish sinuses from capillaries or venules because specific dendritic cells that line the sinuses of lymph nodes are also positive for CD31.1,3,4 Apparent positivity for CD31 could lead to the misinterpretation of sinuses as vascular channels. CD34 is expressed by a variety of cells, and can be detected not only in endothelial cells, but also in reactive fibroblasts and some types of benign and malignant mesenchymal neoplasms.2 Applying anti-CD34 to routinely processed lymph nodes can help to distinguish vascular channels from sinuses because all the sinuses, including peripheral sinuses, would be negative for CD34. In conclusion, it is highly recommended that anti-CD34 should be used together with anti-CD31 to distinguish the vasculature of lymph nodes.
References
- 1.Wacker HH, Frahm SO, Heidebrecht HJ, et al. Sinus-lining cells of the lymph nodes recognized as a dendritic cell type by the new monoclonal antibody Ki-M9. Am J Pathol 1997;151:423–34. [PMC free article] [PubMed] [Google Scholar]
- 2.Miettinen M, Lindenmayer AE, Chaubal A. Endothelial cell markers CD31, CD34, and BNH9 antibody to H- and Y-antigens—evaluation of their specificity and sensitivity in the diagnosis of vascular tumors and comparison with von Willebrand factor. Mod Pathol 1994;7:82–90. [PubMed] [Google Scholar]
- 3.McKenney JK, Weiss SW, Folpe AL. CD31 expression in intratumoral macrophages: a potential diagnostic pitfall. Am J Surg Pathol 2001;25:1167–73. [DOI] [PubMed] [Google Scholar]
- 4.Ruco LP, Pomponi D, Pigott R, et al. Expression and cell distribution of the intercellular adhesion molecule, vascular cell adhesion molecule, endothelial leukocyte adhesion molecule, and endothelial cell adhesion molecule (CD31) in reactive human lymph nodes and in Hodgkin’s disease. Am J Pathol 1992;140:1337–44. [PMC free article] [PubMed] [Google Scholar]