

Primary adenocarcinoma of the bladder accounts for less than 1% of all bladder malignancies.1 Of these, 20–39% are urachal in origin. Urachal adenocarcinoma is more common in men and tends to present in the 5th or 6th decades, although it has been described in a 15 year old girl.2 The common presenting symptoms are haematuria, pain, irritative symptoms, and mucousuria.3 We report a 37 year old woman who presented with a history of irritative voiding symptoms and a suprapubic mass. Five years earlier, she had undergone a laparotomy, partial cystectomy, and excision of a urachal tumour at another centre. Cystoscopy revealed no definite intravesical lesion, apart from a small diverticulum at the site of the previous bladder resection. A bladder biopsy showed a minimal degree of oedema and chronic inflammation, but no other abnormality. A contrast computed tomography scan revealed a mass lesion deep to the anterior abdominal wall, measuring 5 cm in diameter. It was consistent with recurrent carcinoma in the region of the urachal remnant. At laparotomy, we found a mass lesion, situated 10 cm superior to the dome of the bladder, which was attached to the posterior wall of the rectus abdominus muscle. A wide excision of the mass was performed including a large ellipse of skin and rectus muscle. A portion of the dome of the bladder was excised separately to exclude microscopic involvement, and lymph nodes from the omentum were also biopsied.
Histologically, such tumours are often mucinous in phenotype, as was the case in our patient.4 The tumour was multicystic and infiltrated the muscle in an expansile fashion. The epithelium showed only minor atypia, with nuclear hyperchromasia and stratification (fig 1). Comparison of the histology with the resection specimen taken five years earlier showed an identical picture, confirming this as a recurrent urachal adenocarcinoma.
Figure 1.
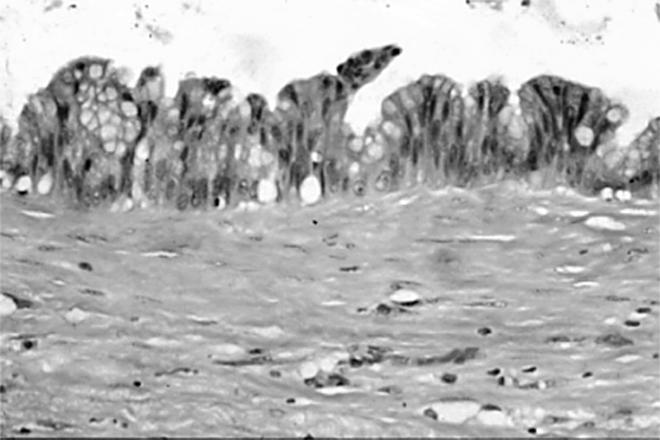
High power photomicrograph of a well differentiated urachal adenocarcinoma showing abundant mucin secretion (upper part).
The prognosis for urachal adenocarcinoma does not differ significantly from non-urachal adenocarcinoma, and is relatively poor, with a five year survival of 37% and a 10 year survival of 17%.4 This may result from the relatively late presentation and advanced stage of these tumours. The treatment is primarily surgical, with extended partial or total cystectomy, and en bloc excision of the urachal mass, urachal tract, and umbilicus advocated.5 These tumours are radioresistant and the results of adjuvant chemotherapy are not yet clear.3
Urachal adenocarcinoma is an uncommon malignancy that often presents late because of its location and relatively non-specific symptoms. This probably results in its poor prognosis. Adequate primary surgery and close follow up is the treatment of choice. Importantly, despite the poor published prognosis and presentation with stage III disease, our patient has survived with only a local recurrence after five years.
References
- 1.Thomas DG, Ward AM, Williams JL. A study of 52 cases of adenocarcinoma of the bladder. Br J Urol 1971;43:4–15. [DOI] [PubMed] [Google Scholar]
- 2.Cornil C, Reynolds CT, Kickham CJ. Carcinoma of the urachus. J Urol 1967;98:93–5. [DOI] [PubMed] [Google Scholar]
- 3.Sheldon CA, Clayman RV, Gonzalez R, et al. Malignant urachal lesions. J Urol 1984;131:1–8. [DOI] [PubMed] [Google Scholar]
- 4.Grignon DJ, Ro JY, Ayala AG, et al. Primary adenocarcinoma of the urinary bladder. A clinicopathologic analysis of 72 cases. Cancer 1991;67:2165–72. [DOI] [PubMed] [Google Scholar]
- 5.Santucci RA, True LD, Lange PH. Is partial cystectomy the treatment of choice for mucinous adenocarcinoma of the urachus [review]? Urology 1997;49:536–40. [DOI] [PubMed] [Google Scholar]