

Abstract
Primary leiomyosarcoma of the testis is an extremely rare condition with only a few reported cases in the literature. None has been reported in men of afrocaribean descent. This report describes the first case of a primary leiomyosarcoma in a mixed race man. Several different immunostains were used to confirm the morphological suggestion of a primary intratesticular smooth muscle tumour. Scrotal ultrasound and abdominal computed tomography imaging were used to exclude paratesticular and retroperitoneal pathology. Where reported, primary intratesticular leiomyosarcoma is described as an indolent tumour with the potential for distant metastases. Its occurrence in younger men is usually associated with anabolic steroid abuse. Although the number of reported cases is very few, radical orchidectomy followed by surveillance appears to be the treatment of choice.
Keywords: primary intratesticular leiomyosarcoma, testis
Primary leiomyosarcoma of the testis is an extremely rare condition with only a few reported cases in the literature.1 We report the first case of a primary leiomyosarcoma in a mixed race man.
CASE REPORT
A 26 year old mixed race (white/afrocaribean) man presented with a four month history of a lump in his left testicle causing mild discomfort. An ultrasound examination confirmed the presence of a 2.2 × 2.0 × 2.5 cm echo poor mass within the upper pole of the left testis, consistent with the radiographic appearance of a testicular tumour. The right testicle and both epididymides were unremarkable and there was no evidence of hydrocele or paratesticular pathology. Liver function and tumour markers, including α fetoprotein, lactate dehydrogenase, and β human chorionic gonadotrophin assays, were all within normal ranges.
He underwent an uncomplicated radical orchidectomy through an inguinal incision for a presumed diagnosis of intratesticular tumour. A subsequent postoperative staging computed tomography scan showed no evidence of local, regional, or distant malignant lymphadenopathy or retroperitoneal disease.
PATHOLOGY
The tumour measured 26 mm in maximum diameter and was situated at the upper pole of the testis abutting the tunica. It had a yellow/orange cut surface and no paratesticular lesions were seen within the specimen. Histologically, the tumour was well circumscribed but lacked a true capsule. It showed a proliferation of spindle cells with elongated, cigar shaped nuclei. The tumour cells were arranged in interlacing bundles (fig 1) with foci of mitotic activity and moderate nuclear pleomorphism. The appearances suggested a malignant tumour of smooth muscle origin or a leiomyosarcoma.
Figure 1.

Spindle cell tumour with nuclear pleomorphism, occasional mitoses and blunt edged nuclei suggesting smooth muscle origin (haematoxylin and eosin stain; original magnification, × 400).
This diagnosis was supported by strongly positive immunostaining for smooth muscle actin (fig 2). Immunostaining for calponin, a highly specific marker for smooth muscle/myoepithelial differentiation, was also positive in the tumour cells. In addition, there was positive staining for desmin and negative staining for caldesmon. This immunoprofile, in conjunction with the morphological appearance, supported a smooth muscle differentiation for the tumour.
Figure 2.
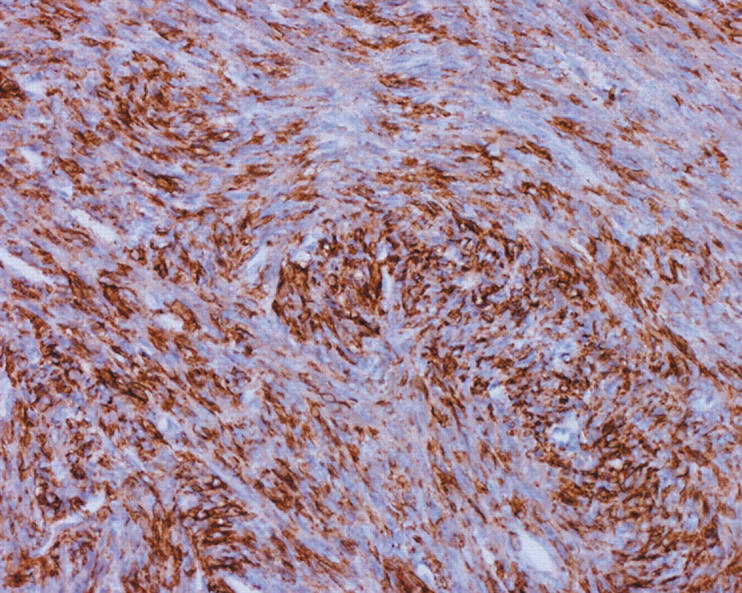
Positive staining with an immunohistochemical marker for smooth muscle (haematoxylin and eosin stain; original magnification, ×200).
Immunostaining for inhibin was negative and excluded a sex cord stromal or Leydig cell origin of the tumour. There was no evidence of germ cell or teratomatous elements. Staining for CD34, CD117, melan A, and HMB45 was also performed and was negative.
DISCUSSION
Controversy exists regarding the classification of these spindle cell tumours within the category of testicular sex cord stromal tumours.2 Theoretically, histiogenesis from undifferentiated gonadal stromal cells is possible. However, descent from smooth muscle cells is equally feasible, and this is supported by the fact that leiomyosarcomas arising from the spermatic cord or epididymal smooth muscle elements form the most common urological sarcomas in adults. The presence of such elements in the tunica albuginea, blood vessels, and testicular parenchyma could provide a site of origin for these rare smooth muscle tumours.
Primary testicular sarcoma is an infrequently reported and rare indolent tumour with the potential for distant metastases.3 A diagnosis should only been made after exclusion of the more commonly seen paratesticular smooth muscle tumours. In this case report, a scrotal ultrasound scan and abdominal computed tomography ruled out paratesticular and retroperitoneal pathology and the morphological appearance, together with the subsequent immunoprofile, strongly supported the diagnosis of a primary intratesticular smooth muscle tumour.
“A diagnosis of primary testicular sarcoma should only been made after exclusion of the more commonly seen paratesticular smooth muscle tumours”
These tumours are exceedingly rare. Where they have been reported, they most often occur in younger men in whom there is an associated history of anabolic steroid abuse.4 Although the number of reported cases is very few, radical orchidectomy followed by surveillance appears to be the treatment of choice for primary leiomyosarcoma of the testis.
Take home messages.
We report the first case of primary leiomyosarcoma of the testis in a man of afrocaribean descent
This tumour is extremely rare and has been described as an indolent tumour with the potential for distant metastases
Its occurrence in younger men is usually associated with anabolic steroid abuse
Radical orchidectomy followed by surveillance appears to be the treatment of choice
REFERENCES
- 1.Yachia D, Auslaender L. Primary leiomyosarcoma of the testis. J Urol 1989;141:955–6. [DOI] [PubMed] [Google Scholar]
- 2.Renshaw AA, Gordon MD, Corless CL. Unclassified sex cord-stromal tumours of the testis with a predominance of spindle cells. Granulosa cell differentiation and reactivity for S-100 protein and smooth muscle actin. Mod Pathol 1997;10:693–700. [PubMed] [Google Scholar]
- 3.Hachi H, Bougtab A, Amhajji R, et al. A case report of testicular leiomyosarcoma. Med Trop (Mars) 2002;62:531–3. [PubMed] [Google Scholar]
- 4.Froeher M, Fischer R, Leike S, et al. Intratesticular leiomyosarcoma in a young man after high doping with oral Turinabol: a case report. Cancer 1999;86:1571–5. [DOI] [PubMed] [Google Scholar]