

The Kayser-Fleischer ring is the single most important diagnostic sign in Wilson's disease; it is found in 95% of patients. Virtually all patients with Kayser-Fleischer rings have neurological manifestations.1 Pseudo rings have been described in other conditions.1 The density of a Kayser-Fleischer ring correlates with the severity of Wilson's disease.2 We describe a rare case of a dense Kayser-Fleischer ring in an asymptomatic patient with an extremely high liver copper content. The recent significant genetic advances, and the clinical implications are discussed.
Case report
At the age of 14 this 23 year old white woman had an evisceration of her left eye for painful rubeotic glaucoma following chronic retinal detachment, resulting from ANA positive iridocyclitis. Her optician referred her because over the past few years, her left prosthetic eye had repeatedly needed an increasingly dense brown ring painted onto it, to match her remaining eye. On examination the visual acuity in the right eye was 6/6 with a heavily pigmented red brown Kayser-Fleischer ring (Fig 1). Her systemic and neurological examinations were normal.
Figure 1.
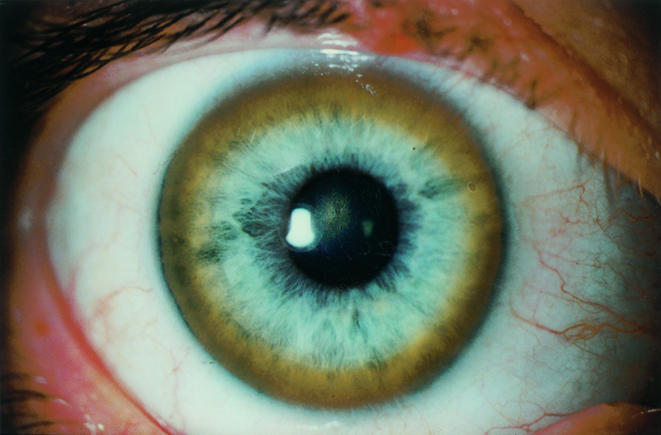
The right eye showing a heavily pigmented red brown Kayser-Fleischer ring.
Baseline biochemistry, liver function, haematology, and cerebral magnetic resonance image (MRI) were normal. She was ANA positive 1 in 20, serum copper 11.6 μmol/l (normal 11–22), and ceruloplasmin 0.15 g/l (normal 0.15–0.45). Twenty four hour urinary copper 9.2 μmol/24 h (normal 0.9 μmol/24 h). Haematoxylin and eosin stained liver biopsy showed normal architecture. Orcein and rhodanine stains showed patchy excessive copper binding protein, and copper within the hepatocytes. The quantified copper content of the sample was hugely elevated at 3000 μg/g (normal 20–50 μg/g).
She was treated with trientine dihydrochloride.3 The Kayser-Fleischer ring initially became denser but has faded considerably over the past 5 years; a thin rim still persists (Fig 2). The patient remains well with no hepatic or neurological manifestations.
Figure 2.
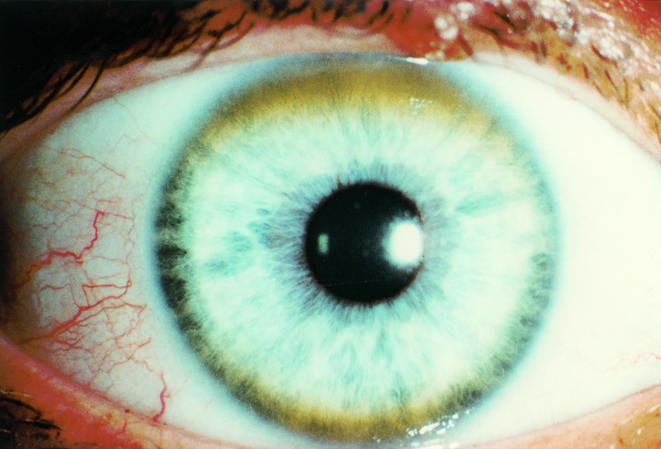
A thin rim still persists 5 years later.
Comment
This patient had an extremely elevated liver copper level, 60 times the normal level. She had to our knowledge the highest ever published liver copper content level over twice the highest level recorded in other publications.4 She had a very dense Kayser-Fleischer ring, but no neurological or hepatic abnormalities. Despite the severity of her condition she remained neurologically asymptomatic with normal liver architecture.
Wilson's disease is inherited as an autosomal recessive trait. The defect has been mapped and sequenced to the long arm of chromosome 13 (13q14.3). The Wilson's gene is responsible for a defective membrane bound P-type ATPase copper transport molecule, ATP7B. This is located in the trans golgi network; the ATPase delivers copper to copper binding ceruloplasmin. During elevated copper levels vesicles containing the ATPase and copper are released by exocytosis into bile. In patients with a defective gene there is an abnormal accumulation and, in comparison, low excretion of stored liver copper.5 These findings contrast with previous theories that Wilson's disease was caused by a defect of apo-ceruloplasmin post-translational modification, and abnormal binding to ceruloplasmin.4
There are a large number of copper binding ATP7B mutations.6 The clinical heterogeneity and overlap of clinical manifestations suggest that locus heterogeneity alone is unlikely to be responsible. It has been hypothesised that there is a subset of pedigrees in which an additional gene is affected other than that for ATP7B.5 Genes encode proteins for detoxification of stored copper—for example, metallothionein, and neutralisation of free radicals such as super oxide dismutase.4,5 This could be a plausible explanation as to why such an extraordinarily high level of copper was bound safely in this patient's liver.
Untreated Wilson's disease has progressive, irreversible consequences, and ultimately causes death.4 The identification of a Kayser-Fleischer ring remains the most important clinical sign for the diagnosis of Wilson's disease.
References
- 1.Finelli PF, Kayser-Fleischer ring: hepatolenticular degeneration (Wilson's disease). Neurology 1995;45:1261–2. [DOI] [PubMed] [Google Scholar]
- 2.Rodman R, Burnstine M, Esmaeli B, et al. Wilson's disease: presymptomatic patients and Kayser-Fleischer rings. Ophthalmic Genet 1997;18:79–85. [DOI] [PubMed] [Google Scholar]
- 3.Tankanow RM. Pathophysiology and treatment of Wilson's disease. Clin Pharm 1991;10:839–49. [PubMed] [Google Scholar]
- 4.Brewer GJ, Yuzbasiyan-Gurkan V, Wilson's disease. Medicine 1992;71:139–64. [DOI] [PubMed] [Google Scholar]
- 5.Camakaris J, Voskoboinik I, Mercer JF. Molecular mechanisms of copper homeostasis. Biochem Biophys Res Commun 1999;261:225–32. [DOI] [PubMed] [Google Scholar]
- 6.Thomas GR, Forbes JR, Roberts EA, et al. The Wilson disease gene: spectrum of mutations and their consequences. Nat Genet 1995;9:210–17. [DOI] [PubMed] [Google Scholar]