

We report a patient with systemic lupus erythematosus (SLE) who developed bilateral ocular ischaemic syndrome in association with orbital inflammation leading to devastating visual loss.
Case report
A 73 year old white woman presented with unilateral acute anterior uveitis and polyarthropathy of the hands, knees, and neck. Over the next 4 years she suffered recurrent anterior uveitis, marginal keratitis, and episcleritis, which were treated with topical steroids. She had bilateral age related cataract and underwent left cataract surgery. Postoperatively, her visual acuities were 6/60 right eye and 6/9 left eye.
She was admitted 7 months later with extensive erythematous, scaly plaques on sun exposed areas and a purpuric eruption over the abdomen, buttocks, and legs. Biopsy of a plaque showed changes consistent with SLE including follicular keratin plugging, epidermal atrophy, degeneration of the basal layer with colloid body formation, basement membrane thickening, myxoid change in the dermis, and periappendageal lymphocyte infiltrates. Biopsy of the purpuric eruption was consistent with a leucocytoclastic vasculitis. Further investigations revealed positive rheumatoid factor (1/100), ANA (1/25), pANCA (1/100), and anti-EN antibodies (1/100). There was reduced C3 and C4, polyclonal increase in IgA and IgM, lymphopenia, thrombocytopenia, and reduced creatinine clearance but no proteinuria. Anticardiolipin antibodies were negative. A diagnosis of SLE was made and oral prednisolone (0.8 mg/kg) was commenced.
Three weeks later she developed a rapid onset of marked bilateral conjunctival and lid oedema, subconjunctival haemorrhage, and proptosis. Visual acuity deteriorated to perception of light in each eye. There was gross restriction of ocular movements. Signs of ocular ischaemia developed in both eyes with corneal oedema, iris neovascularisation, fibrinous anterior uveitis, hyphaema, and raised intraocular pressure (Fig 1). Computed tomography and B-scan ultrasonography of the orbits showed posterior scleritis, choroidal detachment, vitreous haemorrhage, and thickening of the extraocular muscles (Fig 2).
Figure 1.

Anterior segment of right eye showing conjunctival injection, corneal oedema, hyphaema, rubeosis iridis, and cataract
Figure 2.
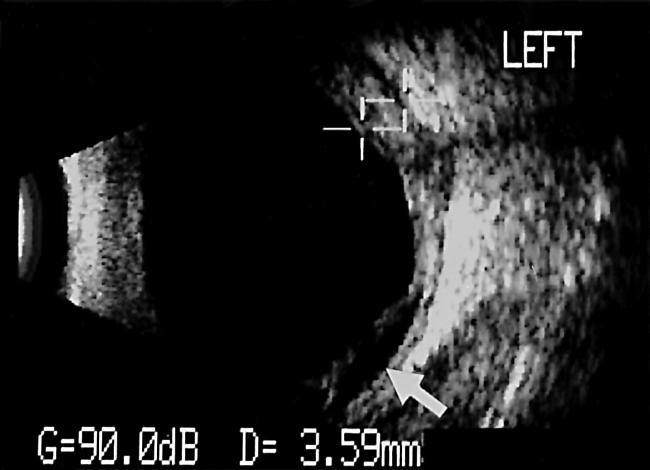
B-scan ultrasound of left eye showing marked posterior scleritis (crosses) and choroidal detachment (arrow).
She was treated with topical dexamethasone 0.1% and carteolol 1%, oral acetazolamide 500 mg daily, intravenous cyclophosphamide (10 mg/kg), and subsequently intravenous immunoglobulin (0.5 g/kg/day for 3 days). Over the following month there was regression of the proptosis, conjunctival and lid oedema, corneal oedema, and fibrinous uveitis. The intraocular pressure was controlled and the visual acuity remained perception of light in each eye. Subsequently, the patient developed pneumonia, VIIth nerve palsy, left sided hemiparesis, and died 7 weeks after admission. Postmortem examination revealed bronchopneumonia, lung abscess, pleural effusions, fibrinous pericarditis, cardiomegaly, and jejunal mucosal haemorrhages. The family did not consent to histopathological examination of the eyes.
Comment
Acute orbital inflammation and orbital myositis leading to proptosis are rare manifestations of SLE.1–7 To our knowledge acute ocular ischaemic syndrome with orbital inflammation is a novel complication of SLE. The ophthalmic manifestations may have resulted from a vasculitis involving the vessels supplying the globe and extraocular muscles. The limitation of ocular movements was most probably the result of mechanical restriction. Although the proptosis, lid and conjunctival oedema improved with immunosuppression, the visual acuity did not recover. This may have been because of irreversible visual loss from optic nerve dysfunction due to ischaemia, compression from the acute orbital inflammation, or secondary to raised intraocular pressure. Close cooperation between ophthalmologist and rheumatologist is essential in the management of these patients, in order to try and prevent blindness.
References
- 1.Brenner EH, Shock JP. Proptosis secondary to systemic lupus erythematosus. Arch Ophthalmol 1974;91:81–2. [DOI] [PubMed] [Google Scholar]
- 2.Wildinson LS, Panush RS. Exophthalmos associated with systemic lupus erythematosus. Arthritis Rheum 1975;18:188–9. [DOI] [PubMed] [Google Scholar]
- 3.Grimson BS, Simons KB. Obital inflammation, myositis and systemic lupus erythematosus. Arch Ophthalmol 1983;101:736–8. [DOI] [PubMed] [Google Scholar]
- 4.Bankhurst AD, Carlow TJ, Reidy RW. Exophthalmos in systemic lupus erythematosus. Ann Ophthalmol 1984;16:669–71. [PubMed] [Google Scholar]
- 5.Fossaluzza V, Dal Mas P. Proptosis and systemic lupus erythematosus. Clin Exp Rheumatol 1987;5:192–3. [PubMed] [Google Scholar]
- 6.Gray RE, Jenkins EA, Hall MA, et al. Recurrent acute proptosis in atypical systemic lupus erythematosus. Clin Rheumatol 1989;8:528–32. [DOI] [PubMed] [Google Scholar]
- 7.Serop S, Vianna RN, Claeys M, et al. Orbital myositis secondary to systemic lupus erythematosus. Acta Ophthalmol 1994;72:520–3. [DOI] [PubMed] [Google Scholar]