

Methanol intoxication can cause severe visual dysfunction and death. Indeed, small amounts of ingested methanol are sufficient to produce acute destruction of parts of the central nervous system leading to permanent neurological dysfunction and irreversible blindness.1–3 More than half of the methanol related morbidity and mortality is classified as accidental and therefore preventable.1 We present, to the best of our knowledge, the first case of a methanol intoxication caused by accidental ingestion of methanol during fire eating (US, fire spitting).
Case report
A 19 year old German patient was admitted to a Spanish university hospital with acute methanol intoxication. The comatose patient had a metabolic acidosis with pH 7.16 and was treated by intravenous ethyl alcohol and bicarbonate. Neurological examination 2 days later with the patient awake revealed extrapyramidal motor disturbances, and computer tomography (CT) scans correspondingly showed basal ganglia infarctions. Visual acuity at this time was light perception in both eyes. Optic discs were reported to be oedematous with dilated peripapillary vessels.
During summertime, the patient had earned his living by fire eating at different Spanish locations. According to the patient, a sudden episode of hiccough during fire eating caused accidental ingestion of denatured alcohol containing methanol.
The patient was transferred to Germany thereafter and presented to our department 6 weeks after the acute intoxication. Visual acuity was light perception. The pupils were dilated and unreactive to light. The eyes were otherwise unremarkable, with the exception of pronounced pale, atrophic optic discs with “pseudoglaucomatous” thinning of the neuroretinal rim area (Fig 1A and B). Acute loss of nerve fibres presumably had induced a “washboard-like pattern” of internal limiting membrane. Nerve fibre layer measurement using GDx technology demonstrated abnormally low values. On magnetic resonance tomography (MRT) imaging, bilateral putamen necrosis typical of methanol intoxication was seen (Fig 2); otherwise the MRT examination was normal. Flash visual evoked potentials (VEPs) were nearly extinguished.
Figure 1.
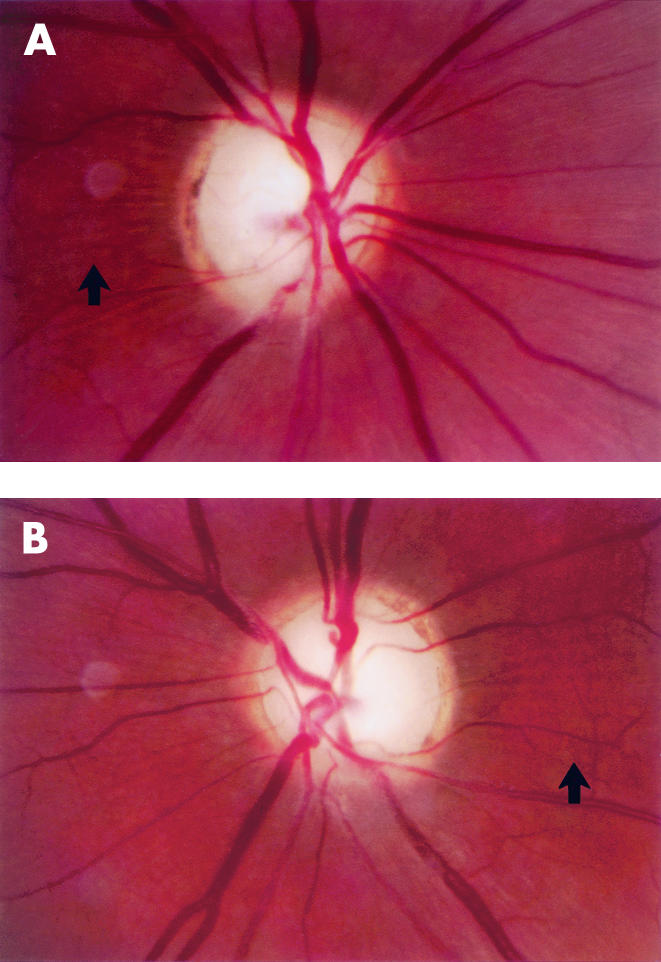
Right (A) and left (B) optic discs of the patient with pseudoglaucomatous optic neuropathy secondary to methanol intoxication (optic disc area both eyes: 2.6 mm2; neuroretinal rim area right eye: 1.1 mm2; left eye: 0.92 mm2). Note intensely pale appearance of the optic disc with alteration of neuroretinal rim configuration and (most likely) pre-existing peripapillary atrophy zone. Note also the “washboard-like” pattern of the internal limiting membrane (arrow) secondary to acute loss of retinal nerve fibres.
Figure 2.
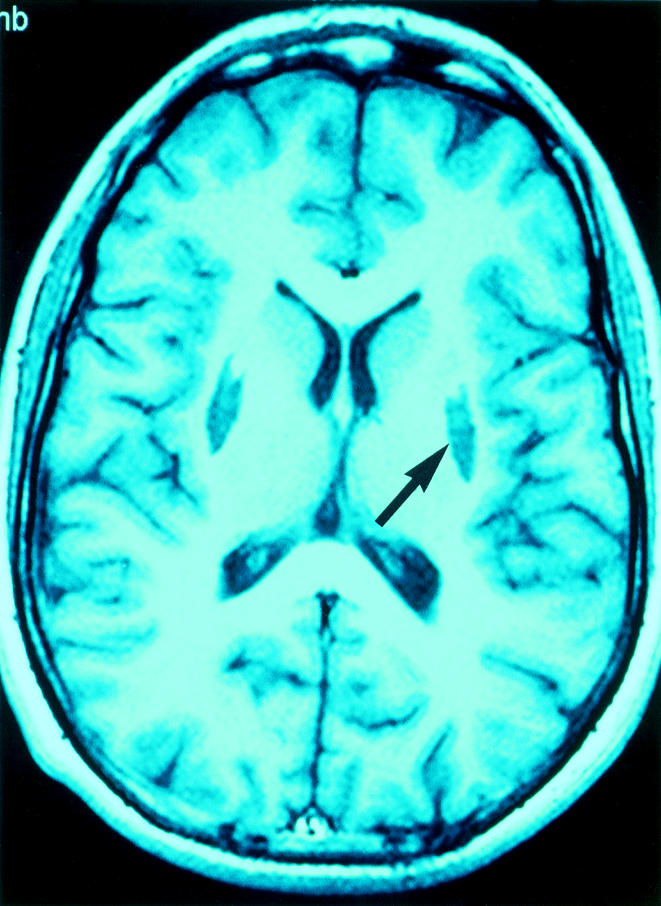
MRT imaging of the patient with methanol intoxication during fire eating (6 weeks after ingestion). Bilateral symmetric necrotic areas in the basal ganglia (putamen; arrow) in the T1 weighted image (hypointense lesions with marginal contrast enhancement) are typical of methanol intoxication.
Comment
As a clear, colourless, volatile liquid with a weak odour, methanol is difficult to differentiate from other forms of alcohols such as ethanol.4,5 Methanol is rapidly absorbed not only after oral ingestion but by inhalation or after cutaneous exposure and becomes oxidised in the liver to formaldehyde and to formic acid, metabolites which are more toxic than methanol itself and which inhibit mitochondrial ATP production. Methanol poisoning can be life threatening and blinding. Early ocular symptoms and signs include photophobia, blurred vision, and painful eye movements as well as sluggish pupil reactions, reduced visual acuity, and optic disc oedema with tortuous retinal vessels. Histopathologically, circumscribed myelin damage behind the lamina cribrosa of the optic nerve has been reported.6 The electrophysiological changes following acute methanol ingestion suggest that methanol affects photoreceptors, Muller cells, and the retrolaminar portion of the optic nerve.7 Treatment is by drug elimination (for example, haemodialysis) and inhibition of metabolism of methanol to toxic formic acid by competitive inhibition of the enzyme alcohol dehydrogenase (ethyl alcohol or fomepizole).8,9
Our patient demonstrates that accidental ingestion of even small amounts of denatured alcohol containing methanol can cause irreversible blindness with intracerebral lesions. For fire eating only denatured alcohol free of methanol should be used.
Acknowledgments
We thank Priv-Doz Dr W Mühlberg, Giftinformationszentrale, Medizinische Klinik II, Klinikum Nürnberg Nord, and Dr A Hahn, Bundesinstitut für gesundheitlichen Verbraucherschutz und Veterinärmedizin, Berlin.
References
- 1.Liu JJ, Daya MR, Mann NC. Methanol-related deaths in Ontario. J Toxicol Clin Toxicol 1999;37:69–73. [DOI] [PubMed] [Google Scholar]
- 2.Kuteifan K, Oesterlé, Tajahmady T, et al. Necrosis and haemorrhage of the putamen in methanol poisoning shown on MRI. Neuroradiology 1998;40:158–60. [DOI] [PubMed] [Google Scholar]
- 3.Onder F, Ilker S, Kansu T, et al. Acute blindness and putaminal necrosis in methanol intoxication. Int Ophthalmol 1998;22:81–4. [DOI] [PubMed] [Google Scholar]
- 4.Seme MT, Summerfelt P, Neitz J, et al. Differential recovery of retinal function after mitochondrial inhibition by methanol intoxication. Invest Ophthalmol Vis Sci 2001;42:834–41. [PubMed] [Google Scholar]
- 5.Eells J, Henry M, Lewandowski M, et al. Development and characterization of a rodent model of methanol-induced retinal and optic nerve toxicity. Neurotoxicology 2000;21:321–30. [PubMed] [Google Scholar]
- 6.Sharpe JA, Hostovsky M, Bilbao JM, et al. Methanol optic neuropathy: a histopathological study. Neurology 1982;32:1093–100. [DOI] [PubMed] [Google Scholar]
- 7.McKellar MJ, Hidajat RR, Elder MJ. Acute ocular methanol toxicity: clinical and electrophysiological features. Aust NZ J Ophthalmol 1997;25:225–30. [DOI] [PubMed] [Google Scholar]
- 8.Brent J, McMartin K, Phillips S, et al. Fomepizole for the treatment of methanol poisoning. N Engl J Med 2001;344:424–9. [DOI] [PubMed] [Google Scholar]
- 9.Girault C, Tamion F, Moritz F, et al. Fomepizole (4-methylpyrazole) in fatal methanol poisoning with early CT scan cerebral lesions. J Toxicol Clin Toxicol 1999;37:777–80. [DOI] [PubMed] [Google Scholar]