

Acute ophthalmic artery occlusion is rare and results in severe ocular dysfunction. We report a patient with Terson’s syndrome who developed an acute ophthalmic artery occlusion after pars plana vitrectomy.
Case report
A 39 year old man suffered a stroke from a subarachnoid haemorrhage on 15 August 2000 and had clipping surgery for a brain aneurysm. The patient presented 3 weeks later, complaining of loss of vision in both eyes. He had had hypertension for 10 years and his sister had a subarachnoid haemorrhage and a cerebral infarction. Visual acuity was hand movements in both eyes, and the intraocular pressure was 10 mm Hg in both eyes. Slit lamp and ophthalmoscopic examination disclosed dense vitreous haemorrhage in both eyes, and the retinas were not visible. B-mode echography detected intravitreous haemorrhage and an incomplete posterior vitreous detachment but the retina was attached bilaterally. The results of other routine laboratory examinations were within normal limits.
Pars plana vitrectomy was performed on the right eye on 30 October after retrobulbar anaesthesia, and the vitreous haemorrhage and epimacular membrane were removed successfully. The retina, retinal vessels, and optic disc appeared normal intraoperatively.
On postoperative day 1, the patient complained of ocular pain in the right eye and the intraocular pressure was 1 mm Hg in the right eye. Slit lamp examination showed marked corneal endothelial folds and fibrinous material filling the anterior chamber. Leakage from the surgical wounds was not observed. Because the hypotony and inflammation did not improve and the right fundus could not be observed, we performed pars plana vitrectomy on 2 November.
The fibrinous material in the anterior chamber and the anterior vitreous were removed. The optic disc appeared pale and swollen. A retinal detachment and a cherry red spot at the macula were not observed; however, the retina appeared pale with multiple blot haemorrhages. The arteries were severely narrowed and the veins were markedly engorged (Fig 1).
Figure 1.
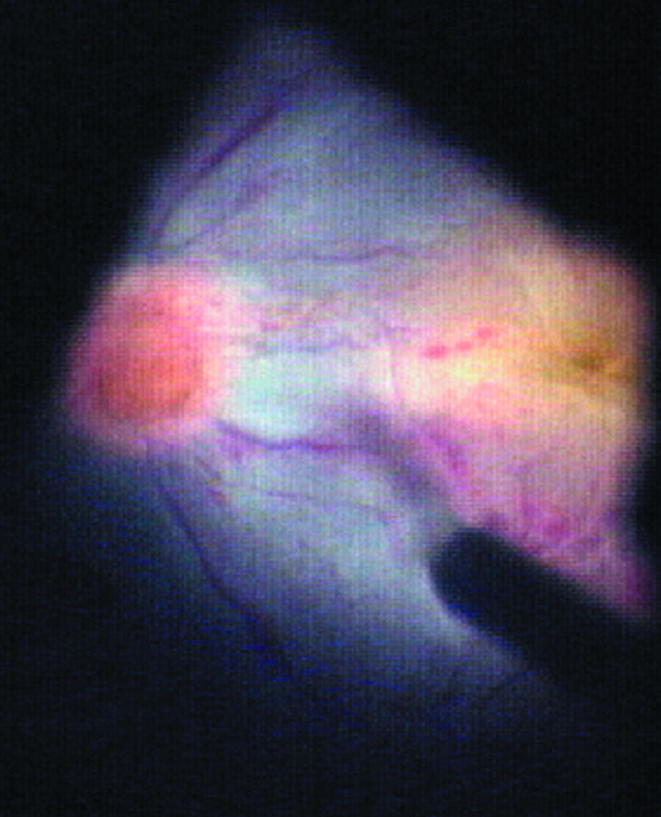
Fundus photograph of the right eye during the second surgery demonstrating disc swelling, whitening of the posterior pole retina, and retinal blot haemorrhage. Retinal arteries are narrowed and retinal veins are engorged.
Fluorescein angiography (FA) demonstrated a delayed entry of fluorescein into the choroid and central retinal artery. The hypotony did not improve after the second surgery, and the pupil was finally occluded in the right eye. The right visual acuity decreased to no light perception.
Colour Doppler sonography, performed 4 months later, revealed that the blood flow velocity was slower in the right (15 cm/s) than in the left ophthalmic artery (25 cm/s). The calibre of the right internal carotid artery was not significantly narrowed, but mixed plaques were attached to the inner wall. Digital subtraction angiography (DSA) of the images obtained immediately after the subarachnoid haemorrhage and 3 weeks after the second surgery, showed good filling of the right ophthalmic artery, indicating that the blood flow into the right eye had been well maintained before the first surgery. From these findings, the patient was diagnosed with an acute ophthalmic artery occlusion following the first vitrectomy.
Comment
There are several causes for the ophthalmic artery occlusion,1–3 and atrial fibrillation and atrial myxoma were excluded in our case, because of normal electrocardiograms and chest x rays. The patient did not have any history of ocular trauma and did not show any symptoms suggesting orbital lesions.
Vasospasms following the subarachnoid haemorrhage can cause ophthalmic artery occlusion; however, such vasospasms usually normalise within 4 weeks after the subarachnoid haemorrhage.4 In our case, the occlusion occurred 3 months after the stroke and immediately after the pars plana vitrectomy, and the DSA findings showed good filling in the right ophthalmic artery, eliminating arteriosclerotic changes in the ophthalmic artery as the cause of the occlusion. Thus, it is most likely that the ophthalmic artery was occluded by an embolus from the atheromatous lesions in the internal carotid artery.
Visual prognosis in Terson’s syndrome is usually good,5 if other retinal disorders are not present. However, patients with this disease usually suffer from other systemic diseases, and we believe ophthalmologists should be aware that an ophthalmic artery occlusion can be associated with vitrectomy in patients with Terson’s syndrome.
References
- 1.Brown GC, Magargal LE, Sergott R. Acute obstruction of the retinal and choroidal circulations. Ophthalmology 1986;93:1373–82. [DOI] [PubMed] [Google Scholar]
- 2.Rafuse PE, Nicolle DA, Hutnik CML, et al. Left atrial myxoma causing ophthalmic artery occlusion. Eye 1997;11:25–9 [DOI] [PubMed] [Google Scholar]
- 3.Bullock JD, Falter RT, Downing JE, et al. Ischemic ophthalmia secondary to an ophthalmic artery occlusion. Am J Ophthalmol 1972;74:486–93. [DOI] [PubMed] [Google Scholar]
- 4.Harders AG, Gilsbach JM. Time course of blood velocity changes related to vasospasm in the circle of Willis measured by transcranial Doppler ultrasound. J Neurosurg 1987;66:718–28. [DOI] [PubMed] [Google Scholar]
- 5.Schults PN, Sobol WM, Weingeist TA. Long-term visual outcome in Terson syndrome. Ophthalmology 1991;98:1814–19. [DOI] [PubMed] [Google Scholar]