

Suppurative keratitis due to Acanthamoeba spp is most commonly associated with poor contact lens hygiene. However, recently there have been reports of keratitis caused by Acanthamoeba spp in the tropics in non-contact lens wearers.1 We report one such case of Acanthamoeba keratitis in Ghana, west Africa.
Case report
A 25 year old male driver (from Accra) reported to a hospital in Bawku, northern Ghana. He presented with symptoms of chronic corneal ulceration (duration of symptoms 31 days) and visual acuity in his affected eye was reduced to perception of hand movements only. The patient did not recall experiencing any trauma to his eye before symptoms. The patient had already taken antibiotics before primary presentation at the hospital but did not bring them with him to clinic and therefore it is not known which they were.
On examination there was a central corneal ulcer (greatest diameter 8 mm) involving more than 50% of the corneal epithelium and more than two thirds infiltrate. The lesion was white, dry in texture, with a well defined margin and raised slough; flare, AC cells, and a posterior corneal abscess were present. Satellite lesions, immune ring, fibrin, keratic precipitates, and hypopyon were absent.
No organisms were isolated from culture on blood agar or Sabouraud agar. Non-nutrient agar was not available at this rural hospital. Corneal ulcer material stained with Gram stain and lactophenol cotton blue mountant was examined, retrospectively, by light microscopy at a tertiary microbiology centre. Cysts, morphologically consistent with the appearance of Acanthamoeba were seen (Fig 1) in the stained smear.
Figure 1.
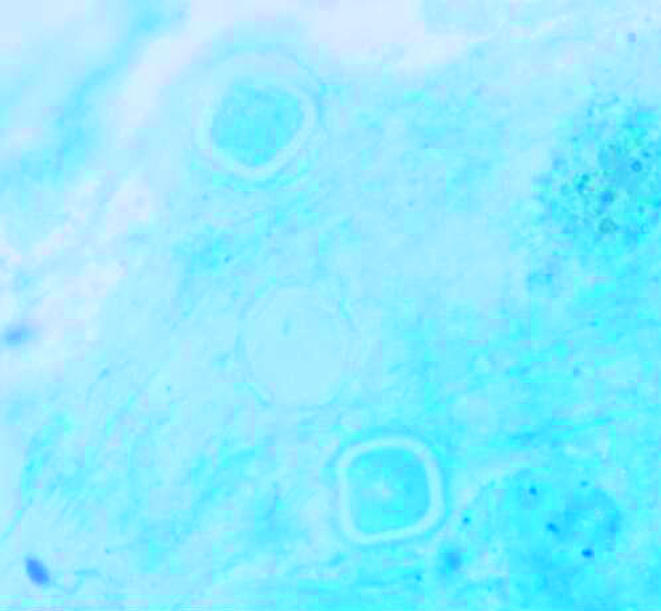
Cysts with the appearance of Acanthamoeba seen in corneal ulcer material.
At the time of presentation the patient was treated empirically with chloramphenicol, gentamicin, and econazole. After 7 days on this regimen the ulcer had not reduced in size. However, there was a reduction of both infiltrate and flare. All other measurements remained the same. At day 21 the ulcer was reported to have improved and a scar had formed (7.4 mm × 7.0 mm). Visual acuity was hand movements only at presentation. The laboratory report was not received before the patient’s final visit and, sadly, the patient could not be traced for further follow up.
Comment
This report illustrates a case of Acanthamoeba keratitis in a non-contact lens wearer in the tropics. Suppurative keratitis due to Acanthamoeba spp is commonly associated with contact lens wear as a result of poor lens hygiene.2 However, increasingly, these ulcers are being reported in developing countries in the tropics in patients who have no history of contact lens wear. Sharma et al described 39 cases of Acanthamoeba keratitis, over a period of 2½12 years; none of the patients was a contact lens wearer. However, 49% of the patients reported experiences of trauma to the affected eye.1
The first cases of Acanthamoeba keratitis in non-contact lens wearers in Africa were reported in Mali by Resnikoff et al.3 This group subsequently reported a further 22 cases between 1990–5.4 However, there have been no other reports, from Africa, of non-trauma related Acanthamoeba ulcers.
The case presented is the first report of a corneal ulcer caused by Acanthamoeba spp in Ghana and highlights the need to consider Acanthamoeba spp as a potential causative agent of chronic keratitis in patients presenting at rural hospitals in the tropics. In addition, the usefulness of simple stains such as lactophenol cotton blue and Gram stain to visualise Acanthamoeba spp is demonstrated as previously described in the literature.5
References
- 1.Sharma S, Garg P, Rao GN. Patient characteristics, diagnosis and treatment of non-contact lens related Acanthamoeba keratitis. Br J Ophthalmol 2000;84:1103–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Radford CF, Lehmann OJ, Dart JKG. Acanthamoeba keratitis: multicentre survey in England 1992–6. Br J Ophthalmol 1998;82:1387–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Resnikoff S, Paniagua-Crespo E, Mjikam JM, et al. First cases of keratitis caused by free-living amoebas of the genus Acanthamoeba diagnosed in Mali. Bull Soc Pathol Exot 1991;84:1016–20. [PubMed] [Google Scholar]
- 4.Quinio D, Flohic AM, Moalic E, et al. Acanthamoeba keratitis: search for a healthy carrier in Mali. Med Trop 2000;60:61–3. [PubMed] [Google Scholar]
- 5.Thomas PA, Kuriakose T. Rapid detection of Acanthamoeba cysts in corneal scrapings by lactophenol cotton blue staining. Arch Ophthalmol 1990;108:168. [DOI] [PubMed] [Google Scholar]