

Down’s syndrome has been reported to be frequently associated with keratoconus, a chronic non-inflammatory corneal disorder leading to scarring and progressive stromal thinning. An incidence of up to 15% in patients with Down’s syndrome was reported in the literature.1 Acute keratoconus or “corneal hydrops” is a frequent feature in these patients leading to a further decrease in visual acuity and a mostly central corneal opacification.2 The spontaneous appearance of a fistula in the acute hydrops state in keratoconus has very rarely been observed. We describe both the clinical and histopathological findings in a patient with Down’s syndrome with acute keratoconus who underwent penetrating keratoplasty following a spontaneous corneal perforation.
Case report
We report on a 59 year old female patient with Down’s syndrome and late stage keratoconus who was referred to our clinic with a 1 day history of corneal hydrops on her left eye. On initial slit lamp examination a marked oedema of the central corneal stroma was apparent with vesicles and bullae in the corneal epithelium and stroma. The lens was cataractous. Visual acuity could not be assessed because of profound mental retardation. Diabetes mellitus had been diagnosed several years ago and was treated by oral antidiabetics. Initial treatment consisted of antibiotic ointment, cycloplegics, and pressure patching.
Three days later the patient returned with a shallow anterior chamber, an epithelial defect and a perforation with aqueous humour leakage in the centre of the corneal swelling. Fibrin was present in the anterior chamber (Fig 1).
Figure 1.
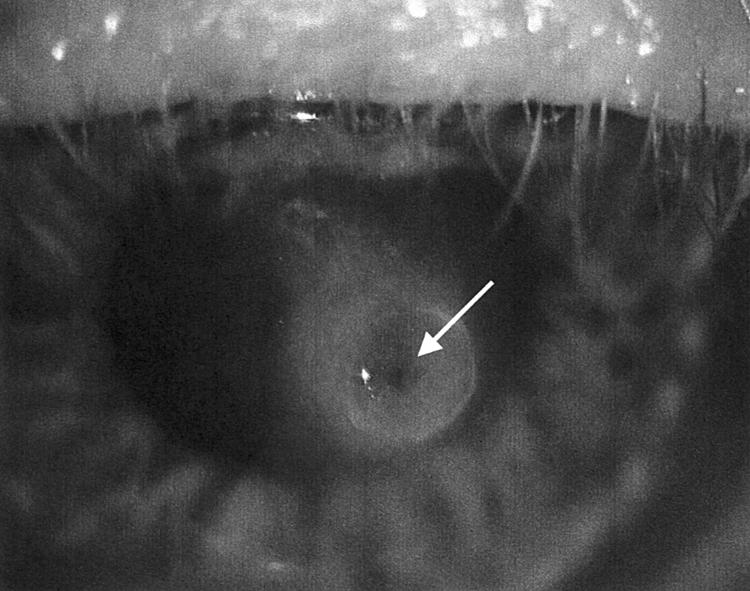
Slit lamp appearance of the cornea, showing an acute hydrops with epithelial defect, perforation with leakage (arrow). Shallow anterior chamber.
Systemic antibiotic treatment was started following admission and a keratoplasty à chaud was planned for the next day. After another 24 hours of pressure patching the anterior chamber had reformed and the outer segment of the fistula was closed. The central part of the cornea had a “nipple-like” aspect. A triple procedure was successfully performed using a 8.25 mm diameter corneal transplant, which had been stored in 31°C organ culture medium. The graft was secured with 24 10-0 nylon interrupted sutures. An extracapsular cataract extraction was performed followed by implantation of an PMMA intraocular lens in the capsular bag. The postoperative period was uneventful. At the 6 month follow up the corneal graft was clear and the intraocular lens well placed. Light microscopy of the excised corneal button revealed features that are regularly found in advanced keratoconus: corneal thinning, “downgrowth” of epithelium in the corneal stroma, breaks and fragmentation of Bowman’s membrane. The cross section displayed a complete fistula, covered by a fibrin-like plug on its outer opening. The surface of the hydrops displayed no corneal epithelium (Fig 2).
Figure 2.
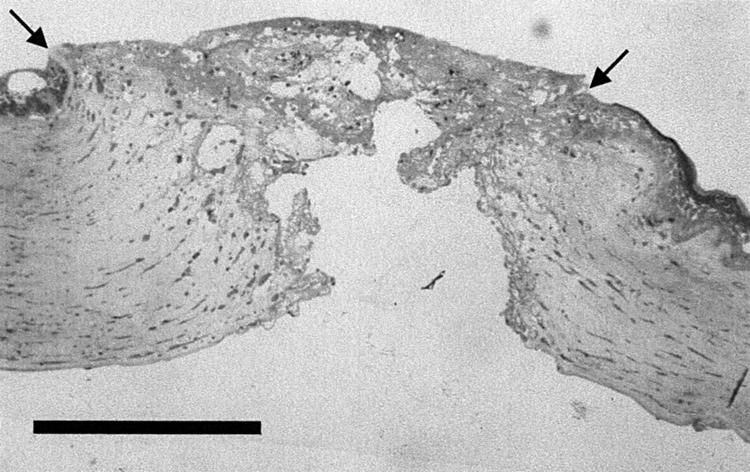
Cross section of the corneal button showing the area of the fistula. Discontinuity of the corneal epithelium (arrows) (azure-II-methylene blue basic fuchsin). Bar = 0.5 mm.
Comment
Corneal hydrops in pre-existing keratoconus is generally caused by the rupture of Descemet’s membrane, followed by an influx of aqueous humour into the weakened corneal stroma that leads to a marked oedema and the formation of cystic spaces. If sufficiently severe, this process may under rare circumstances lead to a complete fistula with leakage of aqueous humour. Very few cases with a spontaneous corneal perforation in acute keratoconus have been reported in the literature.3–8 Three of the patients also suffered from Down’s syndrome. Pierse described the history of a 17 year old boy, who was discovered to have a spontaneously sealed corneal perforation 6 weeks after the onset of acute keratoconus.2 Perforation in a 20 year old female and an 18 year old male patient with corneal hydrops were reported by McElvanney.9 All three patients received a penetrating keratoplasty, with only one of the grafts remaining clear in the long term follow up. Penetrating keratoplasty was also clearly indicated in this reported case of perforation. In general, corneal grafting will be considered in patients with Down’s syndrome and acute keratoconus but, when compared to patients without mental retardation, a much higher complication rate owing to the lack of cooperation has to be taken into consideration.
To the best of our knowledge this is the first report to also present histopathological findings of a fistula following corneal hydrops in keratoconus. Habitual eye rubbing, which is frequently observed in patients with Down’s syndrome and other forms of mental deficiency, has been postulated as an important factor not only for the development of keratoconus itself but also for the progression to the acute condition of the disease.2 As diabetes mellitus is also known to have significant effects on the morphological, metabolic, and physiological aspects of the cornea,10 the coincidence in this particular case may have had an additional detrimental role in the development of this potentially disastrous complication.
References
- 1.Rabinowitz YS. Keratoconus. Surv Ophthalmol 1998;42:297–319. [DOI] [PubMed] [Google Scholar]
- 2.Pierse D, Eustace P. Acute keratoconus in mongols. Br J Ophthalmol 1971;55:50–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ingraham HJ, Donnenfeld ED, Perry HD. Keratoconus with spontaneous perforation of the cornea. Arch Ophthalmol 1991;109:1651–1652. [DOI] [PubMed] [Google Scholar]
- 4.Reis A, Reinhard T, Sundmacher R. Spontane Fistulation bei akutem Keratokonus. Spektrum Augenheilkd 1998;12:197–198. [Google Scholar]
- 5.Musco PS, Aquavella JV. Corneal fistula. Ophthalmic Surg 1987;18:574–576. [PubMed] [Google Scholar]
- 6.Lahoud S, Brownstein S, LaFlamme MY, et al. Keratoconus with spontaneous perforation of the cornea. Can J Ophthalmol 1987;22:230–233. [PubMed] [Google Scholar]
- 7.Grewal S, Laibson PR, Cohen EJ, et al. Acute hydrops in the corneal ectasias:associated factors and outcomes. Trans Am Ophthalmol Soc 1999;97:187–203. [PMC free article] [PubMed] [Google Scholar]
- 8.Rubsamen PE, McLeish WM. Keratoconus with acute hydrops and perforation. Cornea 1991;10:83–84. [PubMed] [Google Scholar]
- 9.McElvanney AM, Adhikary HP. Penetrating keratoplasty in the mentally retarded. Eye 1997;11:786–9. [DOI] [PubMed] [Google Scholar]
- 10.Sanchez-Thorin JC. The cornea in diabetes mellitus. Int Ophthalmol Clin 1998;38:19–36. [PubMed] [Google Scholar]