

Clinical indocyanine green (ICG) angiography has gained an established role in the diagnosis of choroidal neovascularisation (CNV) in age related macular degeneration (AMD).1,2 It is potentially able to localise CNV with greater accuracy compared with fluorescein angiography because it fluoresces in the infrared range, allowing imaging of choroidal pathology through blood and pigment.3 Additionally ICG angiography may better define CNV because of its high protein binding affinity in serum,4 resulting in reduced leak from the CNV. This allows ICG angiography to clearly delineate the feeding vascular supply to the CNV allowing direct ablative thermal laser to precisely target this supply.5
Treatments for CNV, including thermal laser, photodynamic therapy, and macula translocation are all reliant on the ability of the clinician to diagnose accurately the location and nature of CNV. Few clinicopathological data exist to correlate the ICG angiographic appearance of CNV with its histology. The presence of CNV was shown pathologically in an eye with a plaque like hyperfluorescence on ICG angiography shown years previously.6 Lafaut reported the pathology of surgically removed recurrent CNV in two eyes that were preoperatively imaged with ICG angiography.7 The hyperfluorescence of drusen on ICG angiography in the monkey model has been correlated with ICG dye that has been found histologically on infrared fluorescence microscopy.8
In this case report we hope to correlate ICG angiographic findings in a patient with exudative AMD with the histological localisation of ICG to the surgically excised CNV. This will verify that ICG angiographic findings are an accurate representation of the location and nature of the CNV.
Case report
A 71 year old patient with classic subfoveal CNV was recruited into this study to histologically localise ICG dye to excised CNV in AMD. The study was granted institutional research approval by the Sydney Eye Hospital Ethics Committee.
Angiographic evaluation
The patient underwent preoperative imaging with fluorescein and ICG angiography to define the nature and location of the CNV. The angiographic studies were performed on the Heidelberg Scanning Laser Ophthalmoscope (Heidelberg, Germany). Diagnostic studies were performed using 5 ml of 10% fluorescein dye and 25 mg of ICG dye (Pulsion Medical Suppliers, München, Germany).
Follow up angiographic studies were performed one month following surgical removal of the new vessel using standardised methods as outlined above. This was done to confirm the removal of the new vessel.
Surgical procedure
The patient underwent surgical removal of the CNV under assisted peribulbar regional anaesthesia 72 hours later. A three port trans pars plana vitrectomy and removal of the posterior vitreous hyaloid was performed. A small retinotomy adjacent to the CNV was made through which a localised retina detachment was created. The CNV was extracted with subretinal forceps through the retinotomy. Haemostasis was achieved by raising the height of the infusion bottle, increasing intraocular pressure. A fluid-air exchange was carried out after checking the retina periphery for tears.
Histologic localisation of ICG dye
Fifteen minutes before excising the CNV, 50 mg of ICG dye was administered as an intravenous bolus to allow the ICG to bind to the CNV.
The excised specimen was taken immediately to be fixed in 20% dimethyl sulphoxide (Sigma, NSW, Australia) plus 80% adult fixative containing 2% paraformaldehyde in 0.1 M phosphate buffered saline (PBS) (pH 7.4) for 20 minutes.
The tissue was embedded in a small tissue embedding mold with Tissue-Tek OCT 4583 compound embedding medium (Bayer, NSW, Australia) and then rapidly frozen in liquid nitrogen. The frozen tissue block was mounted onto Cryostat Microtome (Leitz, Kryostat 1720, Australia) and 20 µm sections were cut. Sections were collected with geletin-chrom-Alum coated slides and air dried. Sections were then examined for ICG infrared fluorescence or stained with cresyl violet for histologic examination.
Infrared fluorescence microscopy
The technique of infrared fluorescence microscopy to identify ICG fluorescence has been previously described.8 An 810 nm diode laser (Iris Technologies) was used with an excitation filter to stimulate the surgical specimen. A Nikon Eclipse fluorescence microscope with a custom 860 nm barrier filter (Chroma Technologies, Vermont, USA) was used to detect the emitted ICG fluorescence. Paired bright field images with the corresponding infrared fluorescence image were used for orientation of the infrared fluorescence image and recorded digitally.
For histological studies, tissue sections were stained by cresyl violet for 30 seconds, rinsed and dehydrated in graded ethanol, cleared in xylene, and mounted in DePex (BDH, Melbourne, Australia) The sections were examined and photographed under light microscopy.
Angiographic appearances
Fluorescein angiography shows a well defined hyperfluorescent lesion which extends under the fovea consistent with presumed CNV (Fig 1A). ICG angiography shows a hyperfluorescent vascular lesion in the same location (Fig 1B).
Figure 1.

Clinical angiography. (A) Preoperative fluorescein angiography shows that the lesion is well defined and extends into the fovea. (B) Preoperative mid-phase ICG angiogram shows the feeding vascular network that is originating from a peripapillary site. (C) Postoperative fluorescein angiography shows the removal of the CNV. (D) Postoperative ICG angiogram confirms the removal of the CNV.
Postoperative fluorescein and ICG angiography (Fig 1C and D) reveal the absence of the hyperfluorescence confirming that the subfoveal lesion has been excised.
Histologic localisation of ICG
Figure 2A shows the light microscopic image of the surgical specimen stained with cresyl violet. The CNV has a fibrovascular structure. There are associated patchy islands of intact retinal pigment epithelium (RPE) monolayer which are indicated by the arrowheads.
Figure 2.
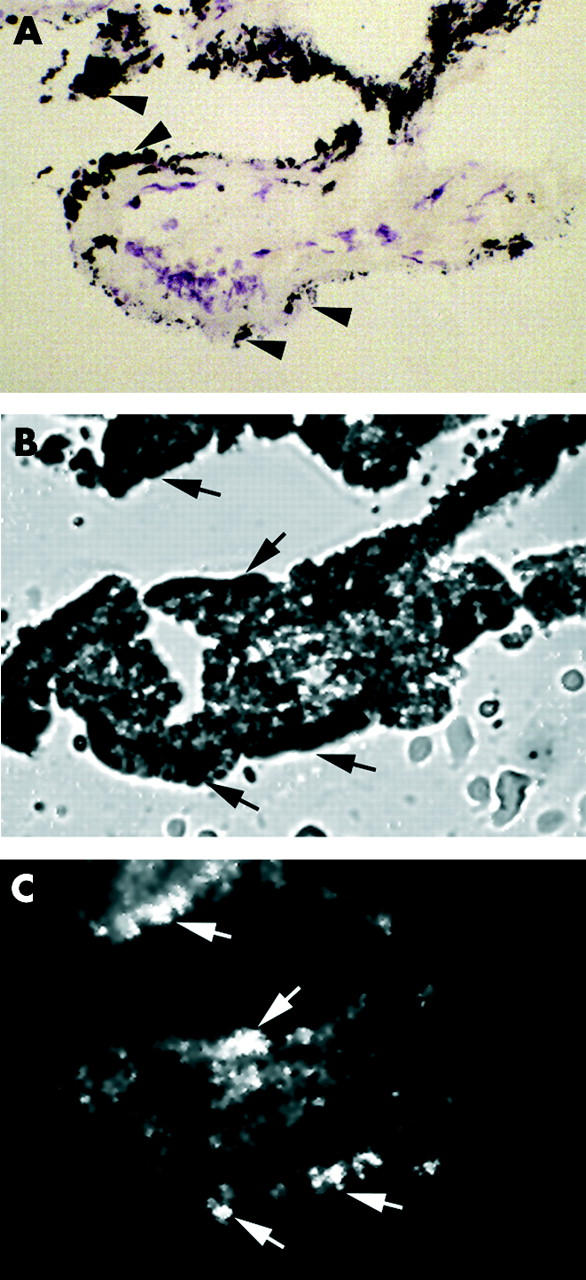
Light and infrared fluorescence microscopy. (A) Light microscopy of excised CNV reveals patchy islands of intact RPE monolayer as indicated by the arrowheads. (B) Bright field image shows the surgical specimen after frozen sectioning. The arrows indicate intact RPE. (C) Infrared fluorescence microscopy demonstrating that ICG fluorescence is localised to the excised CNV. Areas of intact RPE cells are more intensely fluorescent.
Figure 2B is a bright field microscopic image of the surgical specimen. Figure 2C is the corresponding fluorescence microscopic image which shows ICG localised to the excised CNV. Note that the small islands of intact RPE cells indicated by arrows are intensely fluorescent.
Comment
This report provides a direct clinicopathological correlation of CNV defined on ICG angiography, with ICG localised to the excised surgical membrane by infrared fluorescence microscopy. This is unique in that the ICG itself is detected within the excised CNV. This report confirms that hyperfluorescence defined on fluorescein and ICG angiography is consistent with CNV. The hyperfluorescent lesion shown preoperatively is absent following surgical removal of the specimen.
Indocyanine green was histologically localised to the fibrovascular structure of the CNV. It is proposed that ICG enters rapidly into the neovascular complex through its feeding vascular network. The ICG within the feeding vascular network is able to be imaged on the early phase clinical ICG angiography. Subsequently, it is likely that the ICG extravasates through the leaky vessels to bind to the supportive stromal tissues. In this later phase, clinical ICG angiography does not show the feeding vasculature.
Histologically, the CNV was associated with an incomplete layer of RPE cells which were removed with the CNV. This suggests that the CNV in the case studied appeared to be sub-RPE in location. This is consistent with the histopathology of specimens from the Submacular Surgery Trial which would indicate that the CNV in AMD tends to grow under the RPE.9
This report provides information regarding the interaction of ICG with RPE. The intact RPE that were removed with the CNV were intensely fluorescent on infrared fluorescence microscopy. The fluorescence of the RPE was more intense than the fibrovascular tissue. This suggests that that RPE cells accumulate ICG. This finding corroborates the previous histologic localisation studies in the monkey and human model which showed ICG localisation to the RPE.8
The frozen section technique was employed because it allows the water soluble ICG to remain within its in vivo location. Conventional histological processing would cause the ICG to leak through the tissue planes misrepresenting its true position. Previous histological localisation studies in the rat model have been performed using frozen section techniques.10 Preservation of tissue architecture in this study was limited by crush artefact by the subretinal forceps and subsequent extraction from the subretinal space. Additionally, the frozen section processing technique results in tissue expansion and disruption.
This clinicopathological correlation provides the clinician with greater confidence in diagnosing CNV based on ICG angiography.
Acknowledgments
The study was granted institutional research approval by the Sydney Eye Hospital Ethics Committee.
References
- 1.Yannuzzi LA, Slakter JS, Sorenson JA, et al. Digital indocyanine green videoangiography and choroidal neovascularization. Retina 1992;12:191–223. [PubMed] [Google Scholar]
- 2.Lim JI, Sternberg P Jr, Capone A Jr, et al. Selective use of indocyanine green angiography for occult choroidal neovascularization. Am J Ophthalmol 1995;120:75–82. [DOI] [PubMed] [Google Scholar]
- 3.Kramer M, Mimouni K, Priel E, et al. Comparison of fluorescein angiography and indocyanine green angiography for imaging of choroidal neovascularization in hemorrhagic age-related macular degeneration. Am J Ophthalmol 2000;129:495–500. [DOI] [PubMed] [Google Scholar]
- 4.Cherrick GR, Stein SW, Leevy CM, et al. Indocyanine green: observations on its physical properties, plasma decay, and hepatic extraction. J Clin Invest 1960;39:592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Shiraga F, Ojima Y, Matsuo T, et al. Feeder vessel photocoagulation of subfoveal choroidal neovascularization secondary to age-related macular degeneration. Ophthalmology 1998;105:662–9. [DOI] [PubMed] [Google Scholar]
- 6.Chang TS, Freund KB, de la Cruz Z, et al. Clinicopathologic correlation of choroidal neovascularization demonstrated by indocyanine green angiography in a patient with retention of good vision for almost four years. Retina 1994;14:114–24. [DOI] [PubMed] [Google Scholar]
- 7.Lafaut BA, Aisenbrey S, van den Broecke C, et al. Clinicopathological correlation in exudative age-related macular degeneration: recurrent choroidal neovascularization. Graefes Arch Clin Exp Ophthalmol 2001;239:5–11. [DOI] [PubMed] [Google Scholar]
- 8.Chang AA, Morse LS, Handa JT, et al. Histologic localization of indocyanine green dye in aging primate and human ocular tissues with clinical angiographic correlation. Ophthalmology 1998;105:1060–8. [DOI] [PubMed] [Google Scholar]
- 9.Grossniklaus HE, Green WR. Histopathologic and ultrastructural findings of surgically excised choroidal neovascularization. Submacular Surgery Trials Research Group. Arch Ophthalmol 1998;116:745–9. [DOI] [PubMed] [Google Scholar]
- 10.Matsubara T. Histological localization of indocyanine green in the retina and choroid. Jpn J Clin Ophthalmol 1995;49:25–33. [Google Scholar]