

Secondary glaucoma with iris melanocytoma can be successfully managed using sector iridectomy to reduce tumour burden in the anterior chamber. 1, 2 In our case of iris melanocytoma associated with glaucoma, we achieved normalisation of intraocular pressure (IOP) with pupil sparing partial iridectomy. As in previous reports, 1– 3 there was evidence of tumour necrosis, although our tumour exhibited more nuclear pleomorphism than is typical for a melanocytoma.
Case report
A 37 year old white man, with an iris pigmented mass of the left eye discovered at age 17, was followed without incident until he developed acute pain and decreased vision 4 years ago. Review of systems was not remarkable for trauma, surgery, or systemic illness.
Visual acuities were 20/20 in the right eye and hand motion in the left eye. Slit lamp biomicroscopy showed microcystic corneal oedema with 4+ suspended red blood cells in the anterior chamber of the left eye. The thick, deeply pigmented iris mass noted at the 8 to 10:30 o’clock meridian, extended from the angle to within 1 mm of the pupillary margin but did not appear different from baseline. There was slight pupillary distortion and intraocular pressure (IOP) was 55 mm Hg. On gonioscopy the angle was open, although heavily pigmented, except where it was physically obstructed by the mass. Ultrasound biomicroscopy showed no ciliary body involvement. Comprehensive examination of the right eye was unremarkable. IOP of the left eye normalised after starting medical therapy and the hyphaema resolved in 3 months. Glaucoma medications were discontinued without increased IOP.
Eleven months later, vision remained 20/20 but IOP increased to 39 mm Hg in the left eye. Clinically the iris mass appeared unchanged (fig 1A ). Gonioscopy showed a significant increase in trabecular meshwork (TM) pigmentation. A pupil sparing excision of the mass through a limbal incision was performed. Postoperatively, pigment deposition was evident on the corneal endothelium overlying the iridectomy and in the scleral wound (fig 1B ).
Figure 1.
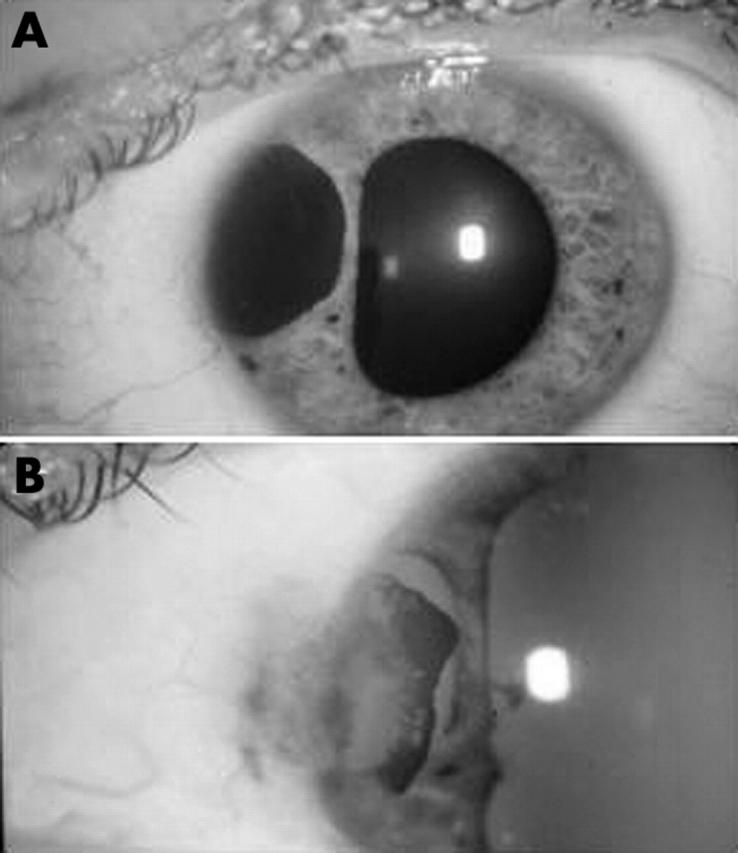
(A) A well defined deeply pigmented mass was present between 8 and 10:30 o’clock positions with distorted pupil of the left eye. (B) After pupil sparing iridectomy, there is pigment deposition on the corneal endothlium and in the scleral wound.
Pathological examination revealed a heavily pigmented tissue devoid of cellular detail and acellular areas consistent with tissue necrosis. Bleached sectioning revealed few cells with typical oval shape, abundant cytoplasm and round nuclei; rather, the majority of cells exhibited marked nuclear pleomorphism (fig 2 ). There was an occasional spindle cell interspersed through the tumour but there were no mitotic spindles. Two ophthalmic pathologists rendered the diagnosis of atypical, necrotic iris melanocytoma.
Figure 2.

Bleached section of the iris pigmented lesion (haematoxylin and eosin, ×100) demonstrates variation in nuclear size and shape. Few plump polyhedra cells with round nuclei and abundant cytoplasm are present (arrow). Some spindle cells are present (*).
Three years postoperatively, vision is 20/20 in the left eye, and IOP is 16 mm Hg without glaucoma therapy. There has been no reorganisation of a pigmented mass. On gonioscopy, there is 1+TM pigmentation.
Comment
Several factors contribute to secondary open angle glaucoma in patients with iris melanocytoma: proximity of the tumour to the filtration apparatus; absence of tumour encapsulation with propensity to pigment dispersion 4 ; tendency for necrotic degeneration within the tumour that further enhances cellular sloughing 1– 3 ; and secondary attraction of macrophages which engulf cellular debris and pigment. 1 Pigment granules, viable and degenerated tumour cells and swollen macrophages obstruct the TM producing increased IOP, a condition coined melanomalytic glaucoma. 5 Excision of the tumour via a pupil sparing partial iridectomy (when possible) accomplishes several goals: it supplies tissue for diagnostic purposes; it reduces tumour volume in the eye, allowing the TM to recover; and provides for an intact pupil.
Abrupt changes in clinical course such as exhibited by our patient raise the possibility of malignant transformation of the lesion. Malignant transformation of iris melanocytoma is rare. 6 Nuclear pleomorphism, a cellular feature associated with malignant behaviour of pigmented tumours, 7 was present in this tumour. Yet definite pathological characteristics of malignancy were absent in our case. There has been no reformation of the lesion or recurrence of glaucoma after 3 years of follow up.
References
- 1. Fineman MS, Eagle RC Jr, Shields JA, et al. Melanocytomalytic glaucoma in eyes with necrotic iris melanocytoma. Ophthalmology 1998;105:492–6. [DOI] [PubMed] [Google Scholar]
- 2. Kiratli H, Bilgic S, Gedik S. Late normalization of melanocytomalytic intraocular pressure elevation following excision of iris melanocytoma. Graefes Arch Clin Exp Ophthalmol 2001;239:712–5. [DOI] [PubMed] [Google Scholar]
- 3. Shields CL, Shields MB, Augsburger JJ. Prevalence and mechanisms of secondary intraocular pressure elevation in eyes with intraocular tumors. Ophthalmology 1987;94:839–46. [DOI] [PubMed] [Google Scholar]
- 4. Yamaguchi K, Shiono T, Mizuno K. Pigment deposition in the anterior segment caused by melanocytoma of the optic disc. Ophthalmologica 1987;194:191–3. [DOI] [PubMed] [Google Scholar]
- 5. Yanoff M, Scheie HG. Melanomalytic glaucoma: report of a case. Arch Ophthalmol 1970;84:471–3. [DOI] [PubMed] [Google Scholar]
- 6. Cialdini AP, Sahel JA, Jalkh AE, et al. Malignant transformation of an iris melanocytoma. A case report. Graefes Arch Clin Exp Ophthalmol 1989;227:348–54. [DOI] [PubMed] [Google Scholar]
- 7. Gamel JW, McLean IW, Foster WD, et al. Uveal melanomas: correlation of cytologic features with prognosis. Cancer 1978;41:1897–901. [DOI] [PubMed] [Google Scholar]