

Abstract
Background: Optokinetic nystagmus (OKN) gain is asymmetrical between temporal to nasal (TN) and nasal to temporal (NT) stimulation in infancy and decreases at older ages. The age at which OKN gain becomes symmetrical and decreases is debated. The aim was to investigate OKN over the whole lifespan in a large sample of healthy subjects.
Methods: In a prospective, cross sectional study OKN was tested monocularly using TN and NT small field stimulation. Stimulation velocity was 15°/s and 30°/s for children aged under 1 year (n = 97), and 15°/s, 30°/s, 45°/s, and 60°/s for older subjects (1–9 years, n = 66; 10–89 years, n = 86). Gain was measured using infrared oculography.
Results: Significant OKN gain asymmetry in favour of TN versus NT stimulation was found during the first 5 months of life (p<0.05). Only at 11 months of age was OKN symmetrical in 100% of the subjects. The percentage of children with symmetrical OKN decreased with increasing stimulus velocity. OKN gain increased in the second and third years (p<0.05 for 15°/s), remained stable until 50 years of age, and showed a small but significant decrease afterwards for the tested velocities (between 6% and 18%, p<0.05).
Conclusions: Infrared oculography is an accurate method to assess OKN, especially in children. Knowledge about change of OKN in healthy subjects could be helpful to interpret OKN in patients with abnormal binocular vision or lesions of the central nervous system.
Keywords: optokinetic nystagmus, age, asymmetry
Optokinetic nystagmus (OKN) consists of a slow eye movement in the direction of the target movement and a fast saccadic eye movement in the opposite direction.1,2 Quality of OKN can be measured with the OKN gain, the ratio of slow phase eye velocity, and stimulus velocity.
In infancy the response of OKN tested monocularly is better when a pattern moves temporally to nasally (TN) than nasally to temporally (NT).3 OKN has been reported to become symmetrical from 3 months of age.4,5,6,7,8,9,10,11
While it has been shown that the ocular system is still developing in preadolescence for smooth pursuit,12 little is known about OKN change after infancy and its later maturation. Lewis13 found that infants showed reduced OKN gain compared to adults in either direction. Several studies have reported a decrease in OKN gain14–20 and a wider variation of OKN gain at older age,14 which possibly contribute to balance problems in the elderly.15
We have investigated changes in OKN related to age in a large group of subjects between infancy and senescence using different stimulus velocities with small field stimulation. We aimed to determine when TN and NT OKN becomes symmetrical, at what age OKN gain is adult-like, and when it decreases later in life. To our knowledge this is the first time that OKN has been investigated over the whole lifespan in one study using the same stimulation and recording techniques.
SUBJECTS AND METHODS
Subjects
The study was approved by the local ethics committee and performed in accordance with tenets of the Declaration of Helsinki. Informed consent was obtained from each subject or their parents.
A total of 249 subjects aged between 18 days and 89 years were investigated (⩽12 months n = 97, 1–9 years n = 66; 10–49 years n = 41 and 50–89 years n = 45). Inclusion criteria were subjects with normal ocular motor system and normal ophthalmological and orthoptic examinations for age. Visual acuity was assessed with Teller acuity cards, picture chart, tumbling E chart, or letter chart depending on the subject’s age. All subjects had a VA of 20/30 or better or Teller acuities within normal limits.21 Exclusion criteria were prematurity (>4 weeks), low birth weight, ophthalmological, neurological or otological diseases, and abnormal binocular functions. Five subjects over 60 years were pseudophakic.
Methods
Generation of OKN
OKN stimulation, eye movement recordings, and analysis were performed with vision monitor equipment (Metrovision, Perenchies, France). Visual stimuli were generated on a monitor measuring 51 cm diagonally placed 40 cm away from the patients (frame rate 120 Hz). The screen’s visual field was 54° horizontally and 41° vertically. OKN was elicited with alternate black (luminance <1 cd/m2) and white (luminance 70 cd/m2) vertical stripes of 2° visual angle (equivalent to a visual acuity of 20/2400). Stripes were presented monocularly to the right eye at constant velocities of 15°/s, 30°/s, 45°/s, or 60°/s either in TN or NT direction in random order, for 40 seconds with 2 minutes intervals between trials.22–24 Infants under 1 year were only investigated at velocities of 15°/s and 30°/s after attempts with higher velocities led to poor recordings. Subjects old enough to cooperate were instructed to look at the centre of the visual field to produce stare nystagmus without following the stripes.
Eye movement recordings
Eye movements were recorded by measuring the position of the corneal reflex with respect to the centre of the pupil with a near infrared illumination of the eye (880 nm). Sampling rate was 60 Hz with a resolution of 10 minutes of arc. Young children were placed in an infant car seat, older children and adults sat on a chair with their head stabilised on a chin headrest. Eye moment recordings were independent of head movements.
Analysis and statistics
Analysis of eye movements included the detection of OKN slow and fast phases and calculation of mean velocity of slow phases. The slope of the best fit regression line plotted across the sample points of the slow phases was used to estimate the velocity. Precision was no greater than 5%. The noise of the velocity measurement was approximately 0.3°/s RMS (company specifications). In young children, measurements were obtained from at least five consecutive slow phases. In cooperative subjects, the mean velocity of consecutive slow phases was measured 5 seconds after stimulus onset during a period of 10 seconds. The early OKN is dominant in humans and has a stable velocity after approximately 0.5 seconds.25 Accordingly, the OKN slow phases had reached a stable velocity over the time period analysed in our experiment.
OKN gain analysis was carried out without knowledge of subjects’ age. ANOVA was performed to compare gains of different groups of age, and was corrected for multiple comparisons using Student-Newman-Keuls tests. To determine the number of subjects with asymmetrical OKN gain the mean TN gain and standard deviation for each age group was calculated. If the NT gain fell outside the plus or minus two standard deviations (95% confidence interval) it was considered asymmetrical. The percentage of subjects falling outside of these limits was determined for each month for the first year of life.
RESULTS
Examples of original recordings of OKN at five different ages are presented in figure 1. At 2 months of age the response for stimulation TN was clearly better than for stimulation NT. At older ages the TN/NT OKN responses were symmetrical.
Figure 1.
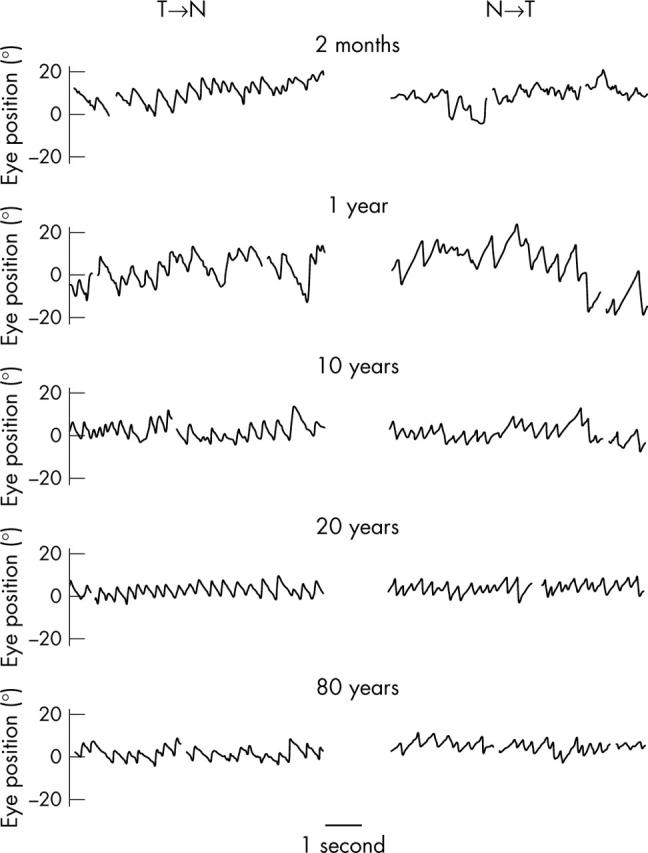
Original recordings of OKN for the right eye with stimulation at velocity of 30°/s from temporal to nasal (TN) (left) and from nasal to temporal (NT) (right) at 2 months (mean TN gain 0.66, mean NT gain 0.31), 1 year (mean TN gain 0.78, mean NT gain 0.73), 10 years (mean TN gain 0.82, mean NT gain 0.8), 20 years (mean TN gain 0.93, mean NT gain 0.92), and 80 years (mean TN gain 0.62, mean NT gain 0.58) of age.
First year of age
A significant asymmetry in favour of the stimulus TN versus NT was found during the first 5 months of life at velocities of 15°/s and 30°/s (p<0.05) (fig 2A). During the first year of life, OKN gain at velocity of 15°/s and 30°/s for stimulus TN was relatively stable with a range from 0.71 to 0.85, and 0.55 to 0.64, respectively. However, OKN gain for stimulus NT progressively increased with a range from 0.38 to 0.78 and 0.25 to 0.57 for 15°/s and 30°/s stimulation, leading to OKN symmetry after the fifth month of age. Symmetrical OKN developed earlier with slower stimulation (table 1). Symmetrical TN/NT OKN was obtained in all subjects at 10 months of age at 15°/s, and at 11 months at 30°/s.
Figure 2.
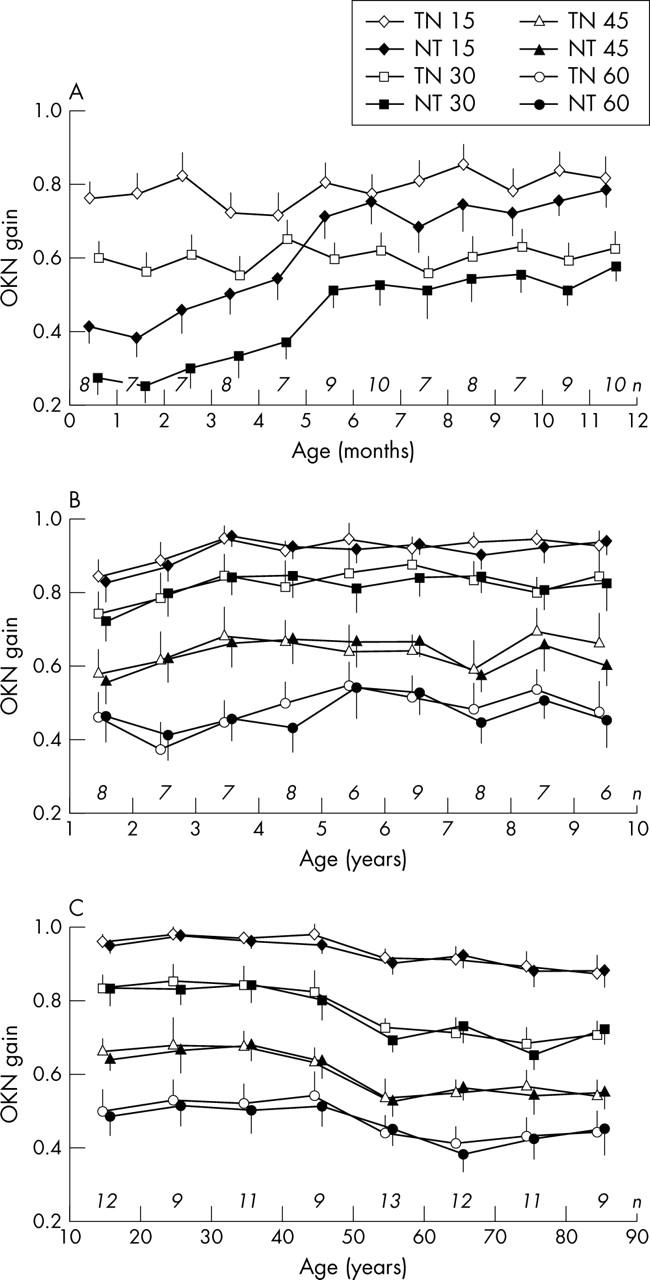
Mean values and standard errors of OKN gains of subjects under 1 year of age (15°/s and 30°/s) (A), between 1 and 9 years of age (B), and between 10 and 89 years of age (C) at stimulation velocities of 15°/s, 30°/s, 45°/s, and 60°/s. Number of examined subjects for each age group are indicated in italics on the X axis.
Table 1.
Number and percentage of subjects with symmetrical OKN for stimulation from temporal to nasal (TN) and from nasal to temporal (NT) at velocities of 15°/s and 30°/s during the first year of life
| Age | TN-NT symmetry 15°/s | TN-NT symmetry 30°/s | ||
| No of subjects | % | No of subjects | % | |
| 1st month | 0/8 | 0 | 0/8 | 0 |
| 2nd month | 0/7 | 0 | 0/7 | 0 |
| 3rd month | 1/7 | 14 | 1/7 | 14 |
| 4th month | 3/8 | 37 | 2/8 | 25 |
| 5th month | 4/7 | 57 | 2/7 | 28 |
| 6th month | 6/9 | 66 | 5/9 | 55 |
| 7th month | 9/10 | 90 | 6/10 | 60 |
| 8th month | 5/7 | 71 | 4/7 | 57 |
| 9th month | 7/8 | 87 | 6/8 | 75 |
| 10th month | 7/7 | 100 | 6/7 | 85 |
| 11th month | 9/9 | 100 | 9/9 | 100 |
| 12th month | 10/10 | 100 | 10/10 | 100 |
During the first year of life, the OKN gain for stimuli TN and NT was significantly higher at velocity of 15°/s than at velocity of 30°/s (p<0.05).
First decade
The results of the changes in OKN gain for TN and NT stimuli at velocities of 15°/s, 30°/s, 45°/s, and 60°/s in 66 children aged between 1 and 9 are plotted in figure 2B.
No TN/NT asymmetry was present. The mean gain appeared to increase with age between 1 year and 3 years for 15°/s (at 1 year: 0.84 for TN and 0.82 for NT; at 3 years: 0.94 for TN and 0.95 for NT), 30°/s (at 1 year: 0.74 for TN and 0. 72 for NT; at 3 years: 0.84 for TN and 0.83 for NT), and 45°/s (at 1 year: 0.57 for TN and 0.55 for NT; at 3 years: 0.68 for TN and 0.65 for NT). Above 3 years, the mean gain remained stable for these stimulus velocities. At 60°/s the mean gain appeared to remain unchanged during the first decade (at 1 year: 0.45 for TN and 0. 46 for NT; at 3 years: 0.44 for TN and 0.45 for NT). We tested whether a significant difference occurred in mean gains between 1–2 year olds and 3–9 year olds and found a significant difference for TN and NT stimulation at 15°/s (p<0.05) but not at other velocities.
In the age group of 1–9 years, the OKN gain for stimuli TN and NT significantly diminished for each increase in stimulus velocity (p<0.05).
10–89 years
Figure 2C shows OKN gains for TN and NT stimuli at the four velocities in the 86 subjects aged between 10 and 89 years. There was no TN/NT asymmetry.
The OKN gain appeared to drop above the age of 50 years at all stimulus velocities. To test this we compared OKN gains for TN and NT stimulation of subjects 10–49 years old (n = 41) with subjects 50–89 years old (n = 45). A significant diminution in OKN gain was found in subjects between 50 and 89 years of age (n = 45) for all velocities (p<0.05). The decrease in gain between 10–49 years and 50–89 years was 7.5% and 6.5% for TN and NT stimuli at 15°/s; 15.4% and 15.4% for TN and NT stimuli at 30°/s; 17.1% and 16.5% for TN and NT stimuli at 45°/s; and 17.4% and 15.3% for TN and NT stimuli at 60°/s.
All ages combined
Figure 3 shows the change of TN and NT OKN gain for the velocities of 15°/s and 30°/s for all ages. They indicate that complete TN/NT symmetry is reached at approximately 1 year of age. OKN gain continues to increase during second and third years stabilising above 3 years of age and remaining stable until approximately 50 years of age significantly declining after this point (p<0.05). OKN gain for stimuli TN and NT was significantly lower in the infants under 1 year compared to older subjects (p<0.05).
Figure 3.
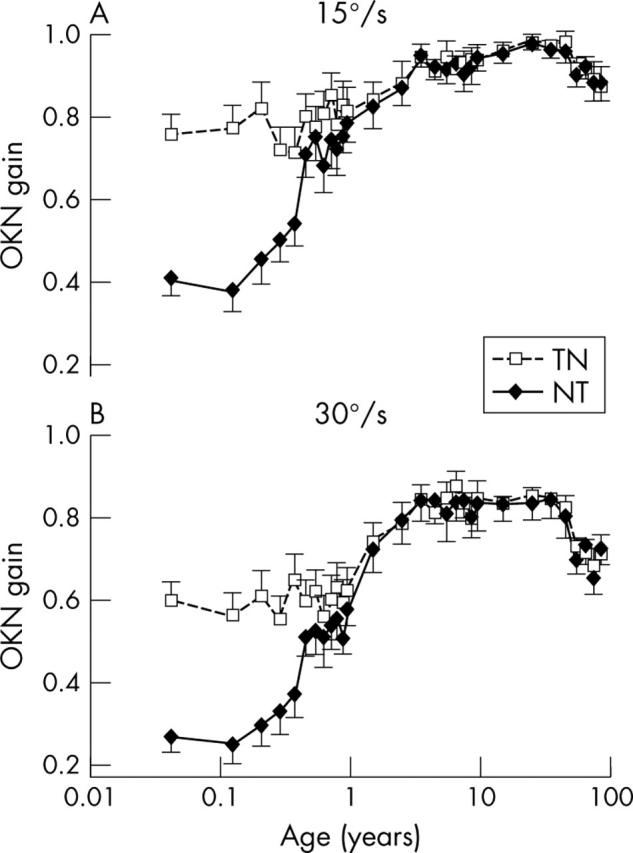
Mean values and standard errors of OKN gains of subjects over the whole age range with stimulation from temporal to nasal (TN) and from nasal to temporal (NT) at velocities of 15°/s (A) and 30°/s (B).
DISCUSSION
OKN symmetry
Our results showed that OKN responses reached symmetry for TN and NT stimulation at the age of 6 months. However, OKN responses were only symmetrical in 100% of subjects at 10–11 months of age, becoming earlier symmetrical with slower stimulus velocity. The development of OKN symmetry resulted from the increase of NT gains, whereas TN gains remained stable during the first year of life.
Different times of appearance of TN/NT symmetry in infants have been described in the literature. Studies based on observation of eye movements found symmetrical OKN at 3 months,4,5 5–6 months,6 12 months,7 or 24 months.8 Studies based on electro-oculography found a symmetrical OKN at 3 months,9 5–6 months,10or later than 7 months.11 In these studies, different stimulus velocities—for example, as low as 12°/s and up to 92°/s,4,6,7,8,9,10,11 were used, partly explaining the variation in the results. In agreement with our results, most studies found that higher velocity stimuli led to later achievement of symmetry. The development of OKN symmetry might also vary with the size of the stimulation field or size and contrast of stripes. For children under 1 year, our method allowed accurate analysis of OKN records at 15°/s and 30°/s, whereas 45°/s and 60°/s gave poor results. This may be explained by the use of small field stimulation in contrast with most other studies.
Development of the fovea in infancy26 is unlikely to have a major role in OKN asymmetries since occlusion of the fovea or age related macula degeneration do not cause asymmetrical OKN.22,27 Conversely, dominant eyes of adult amblyopic subjects with a presumably normal fovea28 often show asymmetrical OKN. Development of symmetrical OKN in infants reflects probably maturation of projections from the retina through the visual cortex to the pretectum.13,29 The direct pathway from the retina to the contralateral nucleus of the optic tract (NOT) and the dorsal terminal nucleus (DTN) is present at birth, and can mediate TN OKN response in the cat.30 The indirect pathway from the retina through the ipsilateral visual cortex to the ipsilateral NOT-DTN is necessary to mediate NT OKN response, and develops later in life leading to the initial OKN asymmetry.31 If normal visual development is disrupted by unequal visual input from both eyes (that is, strabismus) OKN asymmetry can persist.32,33
Age related change of OKN gain
We have shown that before 12 months of age, TN and NT responses were not adult-like. This is in agreement with Lewis13 who found that 6 month olds showed significantly less OKN than adults in either direction. We also found that for slower velocities (15°/s) OKN gain continues to significantly increase during the second and third years, while only a non-significant OKN gain increase was observed for faster velocities. This difference in significance is probably because of the lower variation of OKN gain at 15°/s (note lower standard errors on figures 2B and C) than at 30°/s. Increase in OKN gain during the first decade may partly be due to cortical maturation,34 and possibly caused by improving attention to stimulation.
There is agreement in the literature that ageing decreases OKN gain; however, the age at which OKN gain starts to diminish is controversial. We showed a small but significant OKN gain; reduction for TN and NT stimuli at all tested velocities after 50 years of age. In the literature, most studies compare a population of young and older subjects without reporting the continuous change of the OKN response with ageing.2,15–19 Ura et al16 found a decrease in OKN gain between normal subjects comparing mean ages of 80–30 years. Baloh et al15 reported lower slow phase velocity saturation in normal subjects over 75 years of age compared to younger subjects. Simons and Büttner17 found that OKN maximum velocity decreased considerably with age in control groups after 40 years of age. They also found that maximal smooth pursuit gain and optokinetic after nystagmus (OKAN) was reduced in older age groups. They concluded that both the early component of OKN (related to smooth pursuit) and delayed component (the velocity storage component related to OKAN) were affected in older age. One of the largest series examining the OKN found, in agreement with our results, a decrease of OKN after 50 years of age.20
However, Ura et al16 did not find significant OKN gain differences in elderly subjects with or without vertigo. A possible reason was that only small groups of subjects were investigated and that the normal elderly control group was on average almost a decade older than patients. In our study the standard errors were similar for each age group, and therefore, we cannot confirm the wider variation of OKN response in the elderly.14 In agreement with Magnusson and Pyykkö35 we found no OKN asymmetry with ageing.
As well as OKN gain, other oculomotor functions such as upgaze, saccadic latency, antisaccadic tasks, smooth pursuit, and vestibulo-ocular responses are reduced with ageing.12 While brainstem oculomotor structures are remarkably unaffected by ageing, neuroanatomical changes have been reported for vestibular nuclei, the cerebellum, and cortex in senescence.12 A decrease in cerebellar or cortical neuronal numbers and/or synapses could, therefore, explain reduced OKN gain with ageing. Changes in oculomotor functions could be used to investigate the effect of ageing on structures above the brainstem level.
In summary, to our knowledge, we have performed the first extensive study of OKN evolution in healthy subjects between 18 days and 89 years of age. We found symmetrical OKN responses in infants at 6 months of age. However, only at 11 months of age did 100% of the subjects have symmetrical OKN using higher stimulus velocity. We have shown for the first time that OKN gain increases until the age of 3 years, remains unchanged until 50 years of age, and decreases later in life.
Abbreviations
DTN, dorsal terminal nucleus
NOT, nucleus of the optic tract
NT, nasal to temporal
OKAN, optokinetic after nystagmus
OKN, optokinetic nystagmus
TN, temporal to nasal
REFERENCES
- 1.Westheimer G , McKee S. Visual acuity in the presence of retinal-image motion. J Opt Soc Am 1979;65:847–50. [DOI] [PubMed] [Google Scholar]
- 2.Yee R , Baloh R, Honrubia V. Pathophysiology of optokinetic nystagmus. In: Honrubia V, Brazier M, eds. Nystagmus and vertigo. London: Academic Press, 1982:251–75.
- 3.Teller D , Succop A, Mar C. Infant eye movement asymmetries: stationary counterphase gratings elicit temporal-to-nasal optokinetic nystagmus in two-month-old infants under monocular test conditions. Vis Res 1993;33:1859–64. [DOI] [PubMed] [Google Scholar]
- 4.Atkinson J , Bradick O. Development of optokinetik nystagmus in infants: an indicator of cortical binocularity? In: Fisher D, Monty R, Senders J, eds. Eye movements: cognition and visual perception. Hilldale, NJ: Laurence Erlbaum Associates, 1981:53–64.
- 5.van Hof-van Duin J , Mohn G. Vision in the preterm infant. In: Prechtl H, ed. Continuity of neural functions from prenatal to postnatal life. Philadelphia: Lippincott, 1984:93–114.
- 6.Roy M , Lachapelle P, Lepore F. Maturation of the optokinetic nystagmus as a function of the speed of stimulation in fullterm and preterm infants. Clin Vis Sci 1989;4:357–66. [Google Scholar]
- 7.Lewis T , Maurer D, Holmes R. The development of OKN acuity for nasalward versus temporalward motion. Invest Ophthalmol Vis Sci 1991;32:961. [Google Scholar]
- 8.Lewis T , Maurer D, Chung J, et al. The development of symmetrical OKN in infants: quantification based on OKN acuity for nasalward versus temporalward motion. Vis Res 2000;40:445–53. [DOI] [PubMed] [Google Scholar]
- 9.Mohn G . The development of binocular and monocular optokinetic nystagmus in infants. Invest Ophthalmol Vis Sci 1989;40:49. [Google Scholar]
- 10.Naegele J , Held R. The post-natal development of monocular optokinetic nystagmus in infants. Vis Res 1982;22:341–6. [DOI] [PubMed] [Google Scholar]
- 11.Harris C , Jacobs M, Taylor D. The development of bi-ocular and monocular optokinetic gain from 1 to 7 months. Invest Ophthalmol Visual Sci 1994;35:1829. [Google Scholar]
- 12.Katsanis J , Iacono W, Harris M. Development of ocular functioning in preadolescence, adolescence, and adulthood. Psychophysiology 1998;35:64–72. [PubMed] [Google Scholar]
- 13.Lewis T , Maurer D, Smith R. The development of symmetrical optokinetic nystagmus during infancy. Clin Vis Sci 1992;7:211–18. [Google Scholar]
- 14.Hajioff D , Barr-Hamilton R, Colledge N, et al. Re-evaluation of normative electronystagmographic data in healthy aging. Clin Otolaryngol 2000;25:249–52. [DOI] [PubMed] [Google Scholar]
- 15.Baloh R , Jacobson K, Socotch T. The effect of aging on visual-vestibulo-ocular responses. Exp Brain Res 1993;95:509–16. [DOI] [PubMed] [Google Scholar]
- 16.Ura M , Pfaltz C, Allum J. The effect of age on the visuo- and vestibulo-ocular reflexes of elderly patients with vertigo. Acta Otolaryngol 1991;481:399–402. [DOI] [PubMed] [Google Scholar]
- 17.Simons B , Büttner U. The influence of age on optokinetic nystagmus. Eur Arch Psychiatr Neurol Sci 1985;234:369–73. [DOI] [PubMed] [Google Scholar]
- 18.Kato I , Ishikawa M, Nakamura T. Quantitative assessment of influence of aging on optokinetic nystagmus. Acta Otolaryngol 1994;511:99–103. [DOI] [PubMed] [Google Scholar]
- 19.Matheson A , Darlington C, Smith P. Age-related changes in human optokinetic function. Neuroreport 1998;9:2175–7. [DOI] [PubMed] [Google Scholar]
- 20.Chiba Y , Furuya N. Aging and reference values of the parameters in optokinetic nystagmus. Nippon Jibiinkoka Gabbai Kaiho 1989;92:1416–23. [DOI] [PubMed] [Google Scholar]
- 21.Mayer D , Beiser A, Warner A, et al. Monocular acuity norms for the Teller Acuity Cards between ages one month and four years. Invest Ophthalmol Vis Sci 1995;36:671–85. [PubMed] [Google Scholar]
- 22.Valmaggia C , Charlier J, Gottlob I. Optokinetic nystagmus in patients with central scotomas in age-related macular degeneration. Br J Ophthalmol 2001;85:169–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Valmaggia C , Gottlob I. Optokinetic nystagmus elicited by filling-in in adults with central scotomas. Invest Ophthalmol Vis Sci 2002;43:1804–8. [PubMed] [Google Scholar]
- 24.Valmaggia C , Proudlock F, Gottlob I. Optokinetic nystagmus in strabismus: are asymmetries related to binocularity? Invest Ophthalmol Vis Sci 2003;44:5142–50. [DOI] [PubMed] [Google Scholar]
- 25.Garbutt S , Harris C. A review of optokinetic nystagmus (OKN) in infants and children. Br Orthopt J 1999;56:1–10. [Google Scholar]
- 26.Yuodelis C , Hendrickson A. A qualitative analysis of the human fovea during development. Vis Res 1986;26:847–55. [DOI] [PubMed] [Google Scholar]
- 27.Abadi R , Pantazidou M, Monocular optokinetic nystagmus in humans with age-related macular maculopathy. Br J Ophthalmol 1997;81:123–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Schor C . Subcortical binocular suppression affects the development of latent and optokinetic nystagmus. Am J Optom Physiol Opt 1983;60:481–502. [DOI] [PubMed] [Google Scholar]
- 29.Hoffmann K . Visual inputs relevant for the optokinetic nystagmus in mammals. Prog Brain Res 1986;64:75–84. [DOI] [PubMed] [Google Scholar]
- 30.Hoffmann K . Cortical versus subcortical contribution to the optokinetic reflex in the cat. In: Zee D, Keller E, eds. Functional basis of ocular motility disorders. New York: Pergamon Press, 1982:303–11.
- 31.Simson J , Giolli R, Blanks R. The pretectal nuclear complex and the accessory optic system. In: Buttner-Ennever J, ed. Neuroanatomy of the oculomotor system. New York: Elsevier, 1988:335–64. [PubMed]
- 32.Maurer D , Lewis T, Brent H. Peripheral vision and optokinetic nystagmus in children with unilateral congenital cataract. Behav Brain Res 1983;10:151–61. [DOI] [PubMed] [Google Scholar]
- 33.Westall C , Schor C. Asymmetries of optokinetic nystagmus in amblyopia: the effect of selected retinal stimulation. Vis Res 1985;25:1431–8. [DOI] [PubMed] [Google Scholar]
- 34.Niessen F , Montezer N. The development of visual function. Arch Pediatr 2002;9:1189–94. [DOI] [PubMed] [Google Scholar]
- 35.Magnusson M , Pyykkö I. Velocity and asymmetry of optokinetic nystagmus in evaluation of vestibular lesions. Acta Otolaryngol 1986;102:65–74. [DOI] [PubMed] [Google Scholar]