

Breast cancer has become a leading health concern in the United States, accounting for 30% of all cancers among women.1 Oestrogen is an important hormone involved in the development and growth of breast tumours.2 It has been found that 60–70% of breast cancers have oestrogen receptors.2 Following tumour resection, receptor positive patients are commonly treated with hormone therapy such as tamoxifen. Tamoxifen is a competitive antagonist of oestrogen at its receptor site. It is most often used for postmenopausal patients with oestrogen receptor positive breast cancers. However, tamoxifen also has a partial oestrogen agonist effect which could be detrimental, because it can lead to increased risk for uterine cancer, thromboembolism, and treatment failure.3
The third generation aromatase inhibitors, including anostrozole, letrozole, and vorozole, have emerged as a new treatment for postmenopausal women with oestrogen receptor positive breast cancer. Their mechanism differs from that of tamoxifen as they minimise peripheral conversion of circulating androgen to oestrogen.3 We report one patient with choroidal metastasis from oestrogen receptor positive breast cancer who showed an excellent response to oral aromatase inhibitors.
Case report
A 66 year old woman presented in January 2003 with a 5 month history of flashing lights in the right eye. Her medical history revealed breast cancer, oestrogen receptor positive, treated with modified radical mastectomy and tamoxifen. In 1989, tamoxifen was stopped per the standard 5 year protocol. In October 2002, she developed metastases to the supraclavicular lymph nodes bone and was started on anastrozole.
On examination, visual acuity was 20/60 RE and 20/20 LE. Fundus examination revealed subretinal fluid overlying a solitary amelanotic choroidal metastasis measuring 12 mm in base and 3 mm in thickness (fig 1). The patient was continued on anastrozole. In September 2003, the choroidal metastasis completely regressed with resolution of subretinal fluid (fig 2). Her visual acuity remained 20/40 RE and 20/20 LE.
Figure 1.
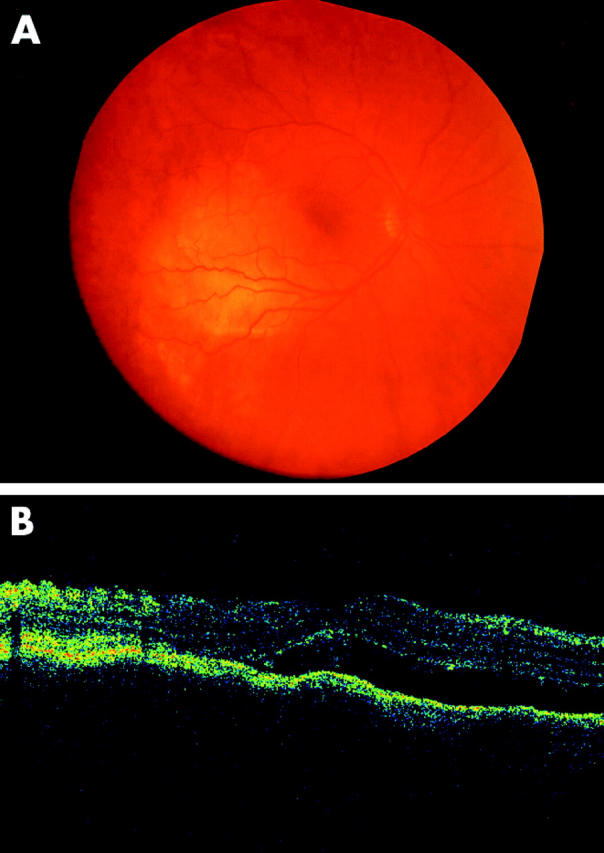
January 2003. (A) Active choroidal metastasis from breast carcinoma at first examination. (B) Optical coherence tomography showing subretinal fluid in the fovea.
Figure 2.
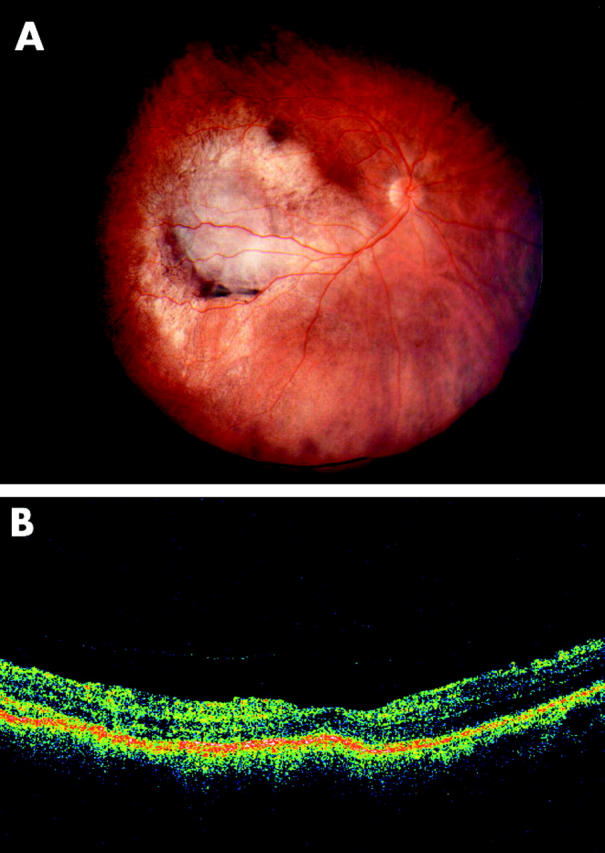
September 2003. (A) Following 9 months of anastrozole treatment, choroidal metastasis has regressed.(B) Optical coherence tomography following 9 months of anastrozole treatment showing resolution of subretinal fluid.
Comment
Uveal metastases are the most common intraocular malignancy. They typically affect the posterior choroids.4 The most common primary sites of cancer are from breast (47%), lung (21%), and gastrointestinal tract (4%).5 Classically, choroidal metastases are yellow, plateau shaped, with secondary subretinal fluid. The treatment of choroidal metastases depends on many factors including location, multiplicity, and activity of each tumour.6,7 Additionally, the projected visual outcome and underlying systemic control is important. In some cases, therapy is limited to the eye, especially if systemic metastases are absent or in remission. In these instances, external beam radiotherapy or plaque radiotherapy are employed.6 In most instances, however, the patient has systemically active metastatic disease so therapy is directed towards treatment of both the ocular and systemic disease using chemotherapy or hormone therapy.6
The most commonly employed hormonal treatment for breast cancer is tamoxifen.2 It is usually employed for postmenopausal patients with breast cancer who display oestrogen receptors. The effect of tamoxifen is due to its anti-oestrogenic activity, by competitive inhibition of oestrogen binding to oestrogen receptors.2 Tamoxifen inhibits the expression of oestrogen regulated genes including growth factors and angiogenic factors secreted by the tumour. Tamoxifen can also induce programmed cell death. Tamoxifen additionally has partial agonist effects, which could be beneficial because it prevents bone demineralisation in postmenopausal women.3 However, these oestrogenic effects are also associated with increased risks of uterine cancer, thromboembolism, and treatment failure.3
Tamoxifen is well tolerated by most patients with breast cancer and only 5% of patients note related menopausal symptoms, such as hot flashes and vaginal discharge.2 Retinopathy has been reported in women with high doses of tamoxifen, but not with conventional doses.
In postmenopausal women the main source of oestrogen is from peripheral conversion of adrenal androgen. New third generation aromatase inhibitors, including anastrozole (Arimidex, Zeneca) and letrozole (Femara, Novartis), act by preventing this conversion, thus lowering circulating oestrogen levels. Studies have shown that they are equal or superior to tamoxifen in clinically efficacy for metastatic breast carcinoma.3 They are well tolerated and have been shown to have important benefits over tamoxifen. Comparative trials indicate that anastrozole has similar adverse effects compared to tamoxifen.8,9 Our patient responded dramatically to aromatase inhibitors after failing to respond to tamoxifen. Based on this case and three other cases with a favourable response we anticipate that aromatase inhibitors could be a promising alternative for patients with choroidal metastases from oestrogen receptor positive breast carcinoma.
Supported in part by the Pan American Ophthalmology Foundation and Retina Research Foundation (Dr ME Manquez), the Eye Tumor Research Foundation, Philadelphia, PA (Dr CL Shields) the Macula Foundation, New York, NY (Dr CL Shields), the Rosenthal Award of the Macula Society (Dr CL Shields), the Paul Kayser International Award of Merit in Retina Research, Houston, TX (Dr JA Shields).
References
- 1.Feig BW, Berger DH, Fuhrman GM. In: Breast cancer. The MD Anderson surgical oncology handbook. Philadelphia: Lippincott Williams and Wilkins, 2003:14.
- 2.Osborne CK. Tamoxifen in the treatment of breast cancer. N Engl J Med 1998;339:1609–18. [DOI] [PubMed] [Google Scholar]
- 3.Smith IE, Dowsett M. Aromatase inhibitors in breast cancer. N Engl J Med 2003;348:2431–42. [DOI] [PubMed] [Google Scholar]
- 4.Shields JA, Shields CL. In: Metastatic tumor to the uvea and retina. Intraocular tumors. A text and atlas. Philadelphia: WB Saunders, 1992:278–320.
- 5.Shields CL, Shields JA, Gross N, et al. Survey of 520 eyes with uveal metastases. Ophthalmology 1997;104:1265–76. [DOI] [PubMed] [Google Scholar]
- 6.Shields CL. Plaque radiotherapy for the management of uveal metastasis. Curr Opin Ophthalmol 1998;9:31–7. [DOI] [PubMed] [Google Scholar]
- 7.Demirci H, Shields CL, Chao AN, et al. Uveal metastasis from breast cancer in 264 patients. Ophthalmology 2003;136:264–71. [DOI] [PubMed] [Google Scholar]
- 8.ATAC. (Arimidex, Tamoxifen Alone or in Combination) Trialists’ Group. Anastrozole alone or in combination with tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomized trial. Lancet 2002;359:2131–9. [DOI] [PubMed] [Google Scholar]
- 9.Mouridsen H, Gershanovich M, Sun Y, et al. Superior efficacy of letrozole versus tamoxifen as first-line therapy for postmenopausal women with advanced breast cancer: results of a phase III study of the International Letrozole Breast Cancer Group. J Clin Oncol 2001;19:2596–606. [DOI] [PubMed] [Google Scholar]