

Three dimensional ultrasound based coronal “C-scan” imaging technique was used to demonstrate optic nerve extension of retinoblastoma. With a clinical diagnosis of retinoblastoma based on clinical evaluation, ultrasound, and computed radiographic tomography, this patient was treated by primary enucleation. Subsequent histopathological evaluation of the enucleated globe revealed three risk factors for metastatic retinoblastoma (including optic nerve extension).1,2 Both systemic chemotherapy and orbital radiation therapy were employed.3
Case report
A 2 year old black female presented with a 1 month history of conjunctival vascular dilation, leucocoria, strabismus, and ptosis involving the right eye. Slit lamp examination revealed a yellow-white tumour filling 70% of the anterior chamber and obscuring view of the posterior segment (fig 1A).
Figure 1.
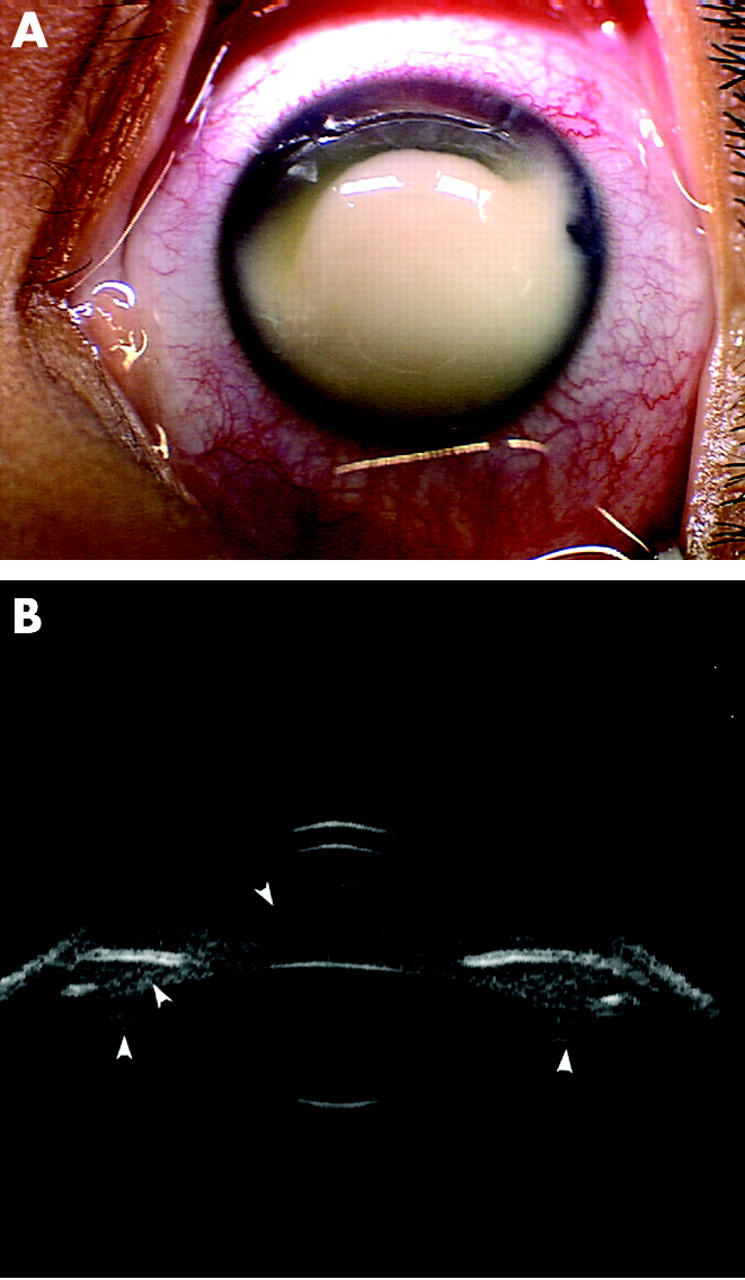
(A) External photograph of the anterior segment filled with retinoblastoma. (B) 35 MHz high frequency ultrasound demonstrates tumour cells in both anterior and posterior chambers, and anterior vitreous (arrowhead).
High frequency ultrasonography (35 MHz) demonstrated the presence of tumour cells in both the anterior and posterior chambers, as well as the vitreous (fig 1B).4 Three dimensional B-scan ultrasonography (3DUS) (12 MHz) revealed a mushroom-shaped retinal detachment and a large endophytic retinoblastoma with orbital shadowing. A V-shaped widening of the optic nerve shadow as it exited the globe was noted (fig 2A). This patient was examined by magnetic resonance imaging (MRI) before enucleation surgery and no optic nerve invasion was noted.
Figure 2.

(A) Three dimensional ultrasound (12 MHz) reconstruction demonstrates a longitudinal view of the V-shaped and widened optic nerve shadow (retinoblastoma infiltrated) as it exits the eye (arrow). Intratumoral calcification (arrowhead) with orbital shadowing (asterisk) consistent with retinoblastoma was noted. (T, temporal, P, posterior, I, inferior). (B) Histopathological evaluation reveals a similar V-shaped, retinoblastoma induced bulging of the optic nerve (arrow) posterior to the globe secondary to diffuse tumour infiltration (haematoxylin and eosin, original magnification, ×40). (C) A posterior coronal “C-scan” image shows an enlarged optic nerve sheath diameter (ONSD) of 6.4 mm (circle). The dark area just superotemporal to the nerve is orbital shadowing caused by retinoblastoma. (D) Higher power view shows a cross section of the distal end of the optic nerve (average ONSD 4.5 mm) with full thickness infiltration by retinoblastoma (haematoxylin and eosin, original magnification, ×100).
Enucleation was subsequently carried out with care to obtain as long an optic nerve stump as possible. There was no difficulty in transsecting the optic nerve. Histopathological sections revealed anterior segment infiltration, massive choroidal involvement, and a corresponding similar V-shaped enlargement of the nerve posterior to the lamina cribrosa (fig 2B). Preoperative coronal C-scan ultrasound views of the optic nerve also demonstrated an enlarged optic nerve sheath diameter (ONSD) (fig 2C). This finding was consistent with full thickness retinoblastoma infiltration of the optic nerve fibre bundles as seen on histopathology (coronal sectioning of the distal end of the transsected optic nerve) (fig 2D).
Subsequent MRI of the brain and lumbar cerebrospinal fluid cytology were interpreted to be normal.
Comment
Retinoblastoma can invade the optic nerve.1,2 Though the entire optic nerve is best evaluated by CT or MRI,5,6 3DUS C-scan imaging has recently been found to be capable of measuring the ONSD. These measurements have been reported from normal healthy subjects and approximate normative values by CT or MRI reports. This technique has also been used in clinical assessment of optic nerve sheath meningiomas.7–9 The relative cost of a three dimensional ophthalmic ultrasound machine is far less than a CT and even less than MRI. Consider that CT and MRI require shielded rooms. Ultrasound examinations are typically shorter than CT or MRI, the ultrasound machine is more mobile, less personnel intensive, and does not require contrast agents.
Optic nerve measurements are based on 3DUS generated coronal C-scan images derived from 97 successive B-scans recorded at 2 degree intervals around the axis of the nerve.9,10 Utilising a representative C-scan image of the nerve, one can trace its outline and obtain an average measurement of the enclosed area. This image is carefully selected from a series of consecutive coronal images of the nerve at a predetermined distance behind the globe. A good correlation between ONSD measurements by C-scan imaging and MRI has been reported.8 The normal ONSD found in healthy adults ranges from 3.9–6 mm by 3DUS, whereas the normative measurement in cadaver eyes is 4 mm.6,7
In this case of retinoblastoma, the measurement obtained 1.5 mm behind the globe was 6.4 mm by 3DUS, and 4.5 mm by histopathology (similar discrepancies have been related to fixation). In this 2 year old patient, both measurements were larger than normal as a result of the mass effect of infiltrated retinoblastoma cells.
Coronal C-scan ultrasound imaging is a new, effective, and relatively inexpensive method to screen for the increased ONSD associated with optic nerve extension of retinoblastoma.
This research was supported by The EyeCare Foundation, Inc and Research to Prevent Blindness, New York, USA.
Competing interests: none declared
References
- 1.Finger PT, Harbour JW, Karcioglu Z. Risk factors for metastasis in retinoblastoma. Surv Ophthalmol 2002;47:1–16. [DOI] [PubMed] [Google Scholar]
- 2.Finger PT, Khoobehi A, Ponce-Contreras MR, et al. Three dimensional ultrasound of retinoblastoma: initial experience. Br J Ophthalmol 2002;86:1136–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wilson MW, Rodriguez-Galindo C, Haik BG, et al. Multiagent chemotherapy as neoadjuvant treatment for multifocal intraocular retinoblastoma. Ophthalmology 2001;108:2106–14. [DOI] [PubMed] [Google Scholar]
- 4.Finger PT, Meskin SW, Wisnicki HJ, et al. High-frequency ultrasound of anterior segment retinoblastoma. Am J Ophthalmol 2004;137:944–6. [DOI] [PubMed] [Google Scholar]
- 5.Daniels DL, Herfkins R, Gager WE, et al. Magnetic resonance imaging of the optic nerves and chiasm. Radiology 1984;152:79–83. [DOI] [PubMed] [Google Scholar]
- 6.Azar-Kia B , Mafee MF, Horowitz SW, et al. CT and MRI of optic nerve and sheath. Semin Ultrasound CTMR 1988;9:443–54. [PubMed] [Google Scholar]
- 7.Garcia JPS, Garcia PT, Rosen RB, et al. A 3D-ultrasound C-scan imaging technique for optic nerve measurements. Ophthalmology 2004;111:1238–43. [DOI] [PubMed] [Google Scholar]
- 8.Garcia JPS Jr, Finger PT, Kurli M, et al. 3D ultrasound coronal “C-scan imaging” for optic nerve sheath meningioma. Br J Ophthalmol 2005;89:238–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Finger PT. Three-dimensional (3D) ultrasonography of the eye. In: Greene R, Byrne SF, eds. Ultrasound of the eye and orbit. Vol II, Chapter 9. Philadelphia: Mosby, 2002:236–43.
- 10.Restori M , Wright JE. C-scan ultrasonography in orbital diagnosis. Br J Ophthalmol 1977;6:735–40. [DOI] [PMC free article] [PubMed] [Google Scholar]