

We report a patient with hypertropia causing diplopia exacerbated by convergence and accommodation.
Case report
A 36 year old man presented with 8 year history of worsening intermittent double vision. Visual acuities were 6/5 in each eye. For near there was manifest left hypertropia and left hyperphoria at distance (fig 1A, table 1). Extraocular movements were full with no overactions. No significant difference in vertical deviation in different gaze positions or cyclotropia was found, the deviation increased on head tilt to the left (table 2). There was no dissociated vertical deviation.1 The angle of deviation varied between 2 and 7 prism dioptres at distance and 24 and 45 prism dioptres at near on repeated examinations. Stereovision was 55 seconds of arc when deviation was prism corrected. The AC/A ratio was normal using gradient method. The vertical fusion range was 13 prism dioptres at distance (9 prism dioptres base-down and 4 prism dioptres base-up).
Figure 1.
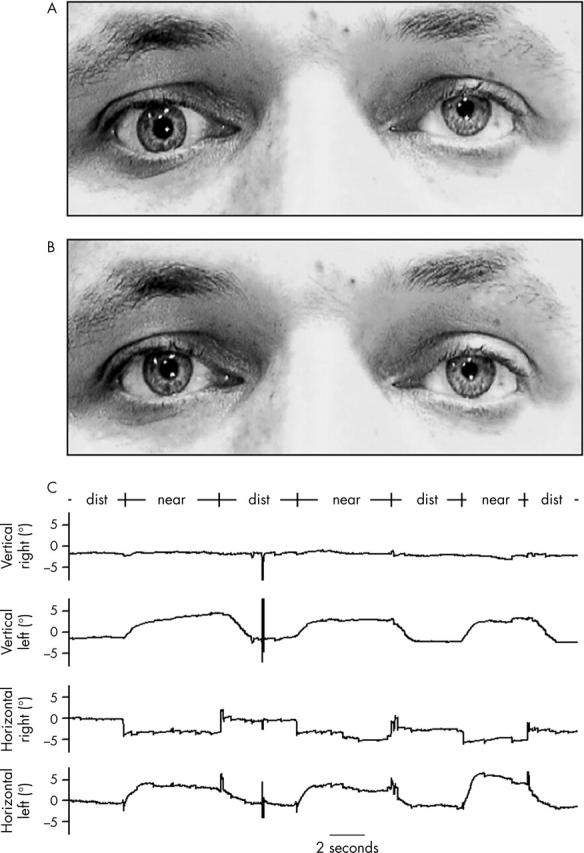
Patient fixating at near with large left over right squint (A) and at distance with no manifest vertical deviation (B). Eye movement recordings of patient during near and distance fixation demonstrating a slow upward drifting of the left eye, which occurred simultaneously with the convergence movement (C).
Table 1.
Angle of deviation on fixation at distance and near measured with the alternating prism cover test
| At 6 metres | 5 prism dioptres L/R* |
| At 6 metres with –1D lens | 8 prism dioptres L/R |
| At 6 metres with –2D lens | 14 prism dioptres L/R |
| At 6 metres with –3D lens | 25 prism dioptres L/R |
| At 33 cm | 30 prism dioptres L/R |
| At 33 cm with +3D lens | 30 prism dioptres L/R |
| At 33 cm with 10 prism dioptres base in | 15 prism dioptres L/R |
*Left over right
Table 2.
Harms Wall measurements in nine directions of gaze (upper panel) and head tilt to the right and left in primary position (lower panel) with left fixation
| Left fixation (red filter over left eye) | |||||||
| Elevation | |||||||
| +2 | 14 L/R | +1 | 12 L/R | +4 | 17 L/R | ||
| 0 | 0 | 0 | |||||
| +2 | 17 L/R | +4 | 15 L/R | +4 | 15 L/R | ||
| Left | 2 Ex | 0 | 2 int | Right | |||
| +3 | 15 L/R | +5 | 14 L/R | +5 | 14 L/R | ||
| 2 Ex | 0 | 0 | |||||
| Depression | 0 | ||||||
| Left fixation | |||||||
| For each direction of gaze the first number indicated the horizontal deviation (ie, +2 = 2 degrees esotropia), the second measurement indicates the vertical deviation (ie, 14 L/R = 14 degrees left over right) and the number under the horizontal and vertical measurements indicated the cyclodeviation (ie, 0 = no cyclodeviation, 2 int = 2 degrees incyclotropia, 2 ex = 2 degrees excyclotropia). | |||||||
| R tilt | L tilt | ||||||
| +14 | 9 L/R | −7 | 20 L/R | ||||
| 0 | 0 | ||||||
The vertical deviation increased on accommodation with concave lenses and the deviation decreased with 10 dioptre base-in prisms at near (table 1). Eye movement recordings are shown in figure 1C. Pupil reactions and fundoscopy were unremarkable. Thyroid functions, thyroid peroxidase and acetylcholine receptor antibodies were normal. Tensilon test was negative. Orbicularis oculi muscle single fibre electromyogram was unremarkable. Neurological examination and magnetic resonance imaging of the brain and orbits were normal.
Comment
Klein-Scharff and Kommerell2 first reported three patients with hypotropia and two with hypertropia modulated by accommodation and/or convergence. In contrast with our patient, +3 dioptre lenses reduced the vertical deviation at near in at least one case. They concluded that the patient had vertical accommodative vergence. Four of five of their cases had additional forms of strabismus.
Gräf and Weinand3 described a case of left hyperphoria increasing on convergence. Use of convex lenses and concave lenses did not change the vertical deviation. Similar to our patient, this child had an increase in vertical deviation when the head was tilted to the side of the hyperphoria/tropia. Gräf has recently attributed this to the unidirectional fusional vertical vergence tonus that developes to compensate for the vertical deviation.4 Gräf5 described three additional cases with vertical accommodative vergence with hypotropia. As in our patients concave lenses at distant fixation increased the vertical deviation. Subsequently, a series of 19 patients with differences in the vertical deviation between near and distance were reviewed.6 Most cases were combined with strabismus sursoadductorius and strabismus deorsoadductorius. In 15 of the 19 patients the vertical deviation increased and in four patients it decreased at near fixation. We agree that supranuclear or internuclear misinnervation most likely explains the connection between elevation and accommodation and convergence.2,3 A more peripheral innervational abnormality can be excluded because there is no elevation of the left eye when the patient is looking to the right (no aberrant innervation between the fibres to the medial rectus and superior rectus).
In our patient it is unclear whether the abnormality was congenital and decompensation of hyperphoria increased symptoms, or whether it was acquired. Increased vertical fusion range argues for a longstanding squint. The history of most patients in the literature1,2 was similar, with slow increase of diplopia and vertical deviation at near over several years. In several patients, combined amblyopia or other strabismus forms—such as dissociated vertical deviation—argue for an early onset of the eye motility problem.2,3 Interestingly, one patient5 seemed to have developed the vertical deviation in combination with convergence after trauma. It is possible that the aberrant re-innervation can be either congenital or acquired. It would be interesting to investigate systematically the influence on near and distance fixation in patients with vertical squint.
References
- 1.Bielschowsky A. Disturbance of the vertical motor muscles of the eye. Arch Ophthalmol 1938;20:175–200. [Google Scholar]
- 2.Klein-Scharff U, Kommerell G. Vertical accommodative vergence. Klin Monatsbl Augenheilkd 1991;199:344–5. [DOI] [PubMed] [Google Scholar]
- 3.Gräf M, Weinand K. Vertical deviation coupled to convergence. Klin Monatsbl Augenheilkd 2000;216:51–3. [DOI] [PubMed] [Google Scholar]
- 4.Graf M, Krzizok T, Kaufmann H. Head-tilt test in unilateral and symmetric bilateral acquired trochlear nerve palsy. Klin Monatsbl Augenheilkd 2005;222:142–9. [DOI] [PubMed] [Google Scholar]
- 5.Gräf M. Drei Fälle von vertikaler accomodativer Vergenz. Klin Monatsbl Augenheilkd 1993;202:136–7. [DOI] [PubMed] [Google Scholar]
- 6.Gräf MH, Rost D, Becker R. Influence of viewing distance on vertical strabismus. Graefes Arch Clin Exp Ophthalmol 2004;242:571–5. [DOI] [PubMed] [Google Scholar]