

Primary intraosseous haemangioma is an uncommon tumour of bone which tends to involve the vertebrae and skull.1,2 Bony orbital lesions are rare with very few case reports in the literature.1,3,4 Simultaneous intradural involvement has never been reported in association with an orbital component. We report an unusual case of capillary haemangioma of the orbital roof with periorbital and dural involvement.
Case report
A 39 year old white male was seen with a 1 year history of painless right upper eyelid swelling and reduced superior visual field. He had marked downward (3 mm), outward (2 mm), and axial (4 mm) displacement of the right globe (fig 1A), with limitation of elevation and 5 dioptres of hypotropia in upgaze. The remaining ocular and systemic evaluation were normal.
Figure 1.

(A) A 39 year old patient showing proptosis and ptosis in the right eye. (B) Gadolinium enhanced coronal T1 fat saturated image through the orbits demonstrates an intraosseous mass in the right orbital roof, with intraorbital and intracranial extension. The intracranial portion was completely extra-axial, with associated dural involvement, as indicated by the thickened and enhancing dura adjacent to the dominant intracranial component. (C) Contrast enhanced coronal computed tomography (CT) image through the orbits demonstrates an intraosseous mass in the right orbital roof, with intraorbital and intracranial extension. Its heterogeneous appearance is the result, in part, of scattered calcifications throughout the mass. Mass effect upon the superior extraocular muscle group is evident.
Contrast enhanced CT and gadolinium enhanced magnetic resonance imaging (MRI) (fig 1B) demonstrated a well circumscribed faintly calcified mass centred within the bony roof of the right orbit. It was homogeneously isointense to grey matter on T1WI, slightly hyperintense on T2WI, and demonstrated marked homogeneous contrast enhancement. Transosseous extension intraorbitally was noted, with displacement of the superior rectus muscle, optic nerve, and globe inferiorly without evidence of invasion or encasement. Transosseous extension of the mass intracranially was completely extra-axial in location, with involvement of the adjacent dura. Provisional diagnosis in the absence of a known primary tumour, was intraosseous meningioma.
The patient underwent right sided frontal craniotomy and orbital osteotomy with piecemeal gross total resection of the right orbital roof, the involved adjacent periorbita, dura and bone.
Grossly, pathological samples including dura (fig 2A) were soft and reddish-light tan coloured in appearance. Microscopic examination (fig 2B) revealed a cellular capillary haemangioma of bone, with periorbital and dural involvement (fig 2D), consisting of thin walled blood vessels with some osteoblastic activity and new bone formation. Tumour immunohistochemistry stains for CD34 (fig 2C), CD31, vimentin, and O13 were positive, confirming a vascular origin.
Figure 2.
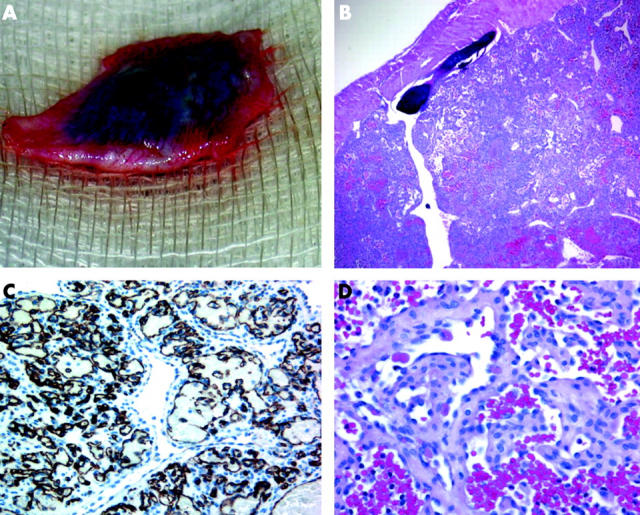
(A) Gross tumour mass showing involved resected dura. (B) HPE: 8×4 magnification showing thin walled blood vessels and osteoblastic activity of intraosseous cellular capillary haemangioma. (C) 6×40 magnification with CD 34 positivity confirming vascular origin. (D) 6×40 dural involvement by capillary haemangioma.
Comment
Intraosseous haemangiomas are benign tumours arising from the intrinsic blood vessels of bone and are two to three times more common in females than males.1,3,5 They are slow growing, accounting for only 0.7–1% of bone tumours, with the most common site being the vertebrae and skull (frontal and parietal).1,3,4 They are typically seen in the adult population, with a peak in the fourth decade, although any age can be affected.1,3–6 Haemangiomas are histopathologically classified as either cavernous (common in the skull and orbit) or capillary (found mainly in vertebrae).1 The pathogenesis of these tumours is unknown.1
The clinical presentation of orbital intraosseous haemangioma is usually a progressive asymptomatic mass which may lead to proptosis, diplopia, optic neuropathy, and ptosis. To date, the largest series3 contained 21 cases, of which four were of the capillary type.3 Though intracranial extension has been noted in the past, intradural lesion is reported only once with calvarial capillary haemangioma (sphenoid)5 but never with orbital invasion.
Plain films typically show bony erosion with scalloped bone giving a “sunburst” appearance.1,4,5 Cavernous and capillary haemangiomas usually have similar imaging findings with differentiation made on histopathological analysis.1
The differential diagnosis for a localised lytic bone lesion with calcifications is wide, including primary bone tumours such as osteosarcoma, chondrosarcoma, meningioma, haemangioma, brown tumour, or infection. Reactive lesions, such as xanthoma of bone, aneurysmal bone cyst, and reparative granuloma are also in the differential. Careful radiological evaluation in combination with clinical history and findings usually allows for differentiation among these different lesions.
With respect to our case, the characteristic high signal intensity on T1 imaging usually seen in vertebral haemangiomas was absent, probably the result of a relatively low fat content.1,2
In our case, atypical dural enhancement on imaging was noted with associated erosion of overlying frontal bone.
Preferred treatment for symptomatic haemangiomas is surgical resection of the entire lesion, with preoperative embolisation.1,3–6 Radiation has been advocated for large and/or unresectable lesions.1,4,7
Competing interests: none declared
References
- 1.Sweet C, Richard S, Bharat Mehta. Primary intraosseous hemangioma of the orbit: CT and MR appearance. AJNR 1997;18:379–84. [PMC free article] [PubMed] [Google Scholar]
- 2.Ross JS, Masaryk TJ, Modic MT, et al. Vertebral hemangioma: MR imaging. Radiology 1987;165:165–9. [DOI] [PubMed] [Google Scholar]
- 3.Relf SJ, Bartley GB, Unni KK. Primary orbital intraosseous hemangioma. Ophthalmology 1991;98:541–7. [PubMed] [Google Scholar]
- 4.Hook SR, Font RL, Mc Cary JA, et al. Intraosseous capillary hemangioma of the frontal bone. Am J Ophthalmol 1987;103:824–7. [DOI] [PubMed] [Google Scholar]
- 5.Khanam H, Maurice HL, Charles LW, et al. Calvarial hemangiomas: report of 2 cases and review of the literature. Surg Neurol 2001;55:67–72. [DOI] [PubMed] [Google Scholar]
- 6.Hornblass A, Zaidman GW. Intraosseous orbital cavernous hemangioma. Ophthalmology 1981;88:1351–5. [DOI] [PubMed] [Google Scholar]
- 7.Pandey SS, Pandey AK. Osseous hemangiomas. Arch Orthop Trauma Surg 1981;99:23–8. [DOI] [PubMed] [Google Scholar]