

Abstract
Objective: This study analysed the relative accuracy of the Bravo wireless and the Slimline catheter-Mark III Digitrapper pH systems in the detection of acid reflux events.
Methods: Twenty five asymptomatic subjects were studied. A Bravo capsule was placed 6 cm above the squamocolumnar junction (SCJ), marked by an endoclip, and a Slimline pH catheter was placed 5 cm above the manometrically localised lower oesophageal sphincter. The distance between the SCJ and each pH electrode was measured fluoroscopically. An in vivo pH reference was established using swallows of orange juice (pH 3.88). Concurrent pH data from the two systems were analysed in Excel spreadsheets.
Results: Significantly more acid reflux events were reported by the Digitrapper system than the Bravo system (117.0 v 41.8). This was not explained by electrode position as there was no difference in median distance between the SCJ and either pH electrode (7.25 cm v 7.08 cm). The dominant source of discrepancy between systems was inaccuracy in electrode calibration and, after adjustment using the in vivo orange juice pH measurement, the discrepancy improved by 40%. However, discrepancy still existed and was most pronounced with short reflux events (1–15 s for the catheter, 1–17 s for the Bravo) associated with minimal intraoesophageal acidity and poor concordance between systems.
Conclusion: Substantially more reflux events were reported by the Digitrapper system compared with the Bravo system; 40% of excess events were attributable to a flawed software scheme for electrode thermal calibration while most of the remainder were brief events with poor reproducibility between systems.
Keywords: pH monitoring, reflux events, Bravo, Slimline
Although ambulatory pH monitoring is considered the most sensitive test for diagnosing gastro-oesophageal reflux disease (GORD), its optimal utilisation in that context remains controversial. In terms of reflux parameters, total oesophageal acid exposure time (the percentage of the day during which oesophageal pH is less than 4) exhibits the strongest correlation with GORD while the number of acid reflux events detected during the study appears to have the weakest correlation.1 None the less, defining the timing and severity of acid reflux events is still one of the most important aspects of pH monitoring because it provides a means of establishing a temporal relationship between symptoms and acid reflux. Indeed, several such symptom association indices are in widespread clinical use, evident by their being a common feature of all ambulatory oesophageal pH monitoring analysis software.
An obvious prerequisite for the utility and reproducibility of an index gauging the strength of association between acid reflux and symptom perception is accurate detection of acid reflux events. Significant overreporting or underreporting of acid reflux events will systematically weaken any legitimate symptom-reflux association scheme. Despite this importance, the accuracy with which ambulatory pH monitoring systems detect and report reflux events has been the object of surprisingly little scrutiny. What evidence does exist suggests that reproducibility and/or accuracy may be suboptimal. An early investigation using two oesophageal pH electrodes placed simultaneously at the same position within the oesophagus revealed substantial variability between the two pH tracings.2 More recently, studies evaluating simultaneous oesophageal pH recordings using the Bravo pH system and various antimony catheter systems have revealed significant differences in the reported oesophageal acid exposure time.3–5 Given these findings, it seems somewhat likely that the two systems will also report discrepant results with respect to the detection of acid reflux events. Thus the aim of this study was to compare the performance of the Bravo pH monitoring system with that of the most widely used catheter based system, the Slimline catheter with the Mark III Digitrapper (Medtronic Inc., Shoreview, Minnesota, USA), in detecting acid reflux events.
METHODS
Subjects
Twenty five healthy asymptomatic volunteers without oesophagitis (20 males, five females, 19–35 years old) participated in the study. Subjects were enrolled from the gastrointestinal diagnostic laboratory at Northwestern Memorial Hospital. The study protocol was approved by the Northwestern University Institutional Review Board and informed consent was obtained from each subject.
Upper endoscopy
Upper endoscopy was performed with a 27 French endoscope in the left lateral decubitus position to localise the squamocolumnar junction (SCJ). During endoscopy, which was done either unsedated or under moderate sedation with 1–4 mg of midazolam, the position of the SCJ was marked by placement of an 11 mm stainless steel clip (Olympus HX-SLR-1 clip fixing device, Japan).
Bravo capsule pH monitoring
Prior to placement, the Bravo pH capsule (Medtronic Inc.) was activated by a magnetic switch and calibrated according to the manufacturer’s protocol (Medtronic Inc.) at 25°C. In the process, the capsule and receiver were also checked to confirm correct functioning of data transmission. The Bravo delivery system was passed orally with subjects in the left lateral decubitus position and positioned 6 cm proximal to the SCJ. The capsule was deployed in a standard fashion.6 Five different Bravo receivers were used during this study and rotated based on availability.
Digitrapper catheter pH monitoring
After Bravo capsule placement, a dual sensor antimony pH catheter (Slimline; Medtronic Inc.) connected to a portable digital data recorder (Mark III Digitrapper; Medtronic Inc.) was placed. A new catheter electrode was used for each subject. Prior to passage, the pH catheter was calibrated at 25°C in pH 7.01 and pH 1.07 buffer solutions as per the manufacturer’s protocol (Medtronic Inc.). The catheter pH electrode was then passed transnasally with positioning established based on interpretation of the prior day’s high resolution manometric evaluation to identify the proximal margin of the LOS. Three different Digitrapper data recorders were used during this study and rotated according to availability.
Experimental protocol
Endoscopy with SCJ clipping was performed on day 1. On day 2, subjects returned at 7:00am for placement of both pH monitoring systems. First, the Bravo system was placed (unsedated) by one investigator (JEP). Then, a second investigator, blinded to the endoscopic findings, placed the Slimline pH catheter 5 cm above the proximal margin of the LOS (CB). The pH catheter was secured to the nose with tape and the subject was taken to fluoroscopy. The subject was then shielded below the umbilicus with a lead apron and positioned upright within the imaging field of a C-arm fluoroscope (Easy Diagnostics, Phillips Medical Systems, Shelton, Connecticut, USA). Images were obtained during normal respiration while the subject refrained from swallowing. The subject then returned to the manometry laboratory and consumed 100 ml of orange juice at room temperature (Pure; Home Juice Co., Melrose PK, Illinois, USA). Subjects then left the laboratory with instructions to carry out normal daily activities. Subjects returned at 7:00am on day 3 at which time they underwent repeat fluoroscopic imaging and consumed a second 100 ml glass of orange juice. The Slimline pH catheter was then removed and data from the Mark III Digitrapper were uploaded to a designated computer using PolygramNet software (Medtronic Inc.). The subject then left the laboratory again and underwent an additional 24 hours of Bravo pH monitoring, returning the following day for data upload to a computer via Datalink (Medtronic Inc.) that is compatible with Windows 95/98/2000 NT.
Data analysis
pH electrode placement
The distance between the SCJ and the pH electrode for both the catheter and Bravo capsule was measured from digitised fluoroscopic images that were uploaded to a Macintosh Computer. NIH image software was used to measure the distance between the metal clip at the SCJ and each pH electrode on day 1 and day 2. A vertebra was used as a spatial reference and the Bravo capsule (2.6 cm in length) was used to correct for magnification. Measurements were made by a single investigator (QZ) who was not involved in placement of either pH electrode and was blinded to the results of the pH study.
Detection of acid reflux events (software reported and manual reanalysis)
As would be done for a routine clinical study, the manufacturer’s software for both the Mark III Digitrapper catheter system and the Bravo system (PolygramNet; Medtronic Inc.) was utilised to ascertain the number of acid reflux events during the day when both electrodes were in place. Reflux event parameters for the Mark III Digitrapper system were set at a sampling frequency of every four seconds and defined as a single measurement less than pH 4. In addition, the oscillatory index was set as 3.75–4.25. Reflux event parameters for the Bravo system were set at a sampling frequency of every six seconds and defined as a single measurement less than pH 4. Similar to the Mark III Digitrapper system, the oscillatory index was set as 3.75–4.25.
The number of acid reflux events were also evaluated by manual reanalysis of the pH data points transferred from the two data loggers. Data from both recording systems were converted to ASCII files and transferred to patient specific Excel spreadsheets. To facilitate precise synchronisation, both files were expanded to a one second frequency. This required duplicating each Digitrapper value four times and each Bravo value six times because of the different sampling frequencies of the two systems. The net result was a spreadsheet with second-by-second simultaneous Digitrapper and Bravo pH data over 24 hours (approximately 86 000 paired data points).
The synchronised simultaneous data spreadsheets were further analysed in a systematic fashion to determine the extent of discrepancy between the recording systems attributable to missing data. Each system had a unique code for missing data; in the Digitrapper these were recorded as pH values <0.5 and in the Bravo system as −0.05. Missing data with the catheter system were potentially attributable to poor electrode contact, software faults, or hardware faults, while with the Bravo system, poor signal reception represented an additional (and most likely) cause of missing data.
Offset adjustment
Recognising the importance of electrode calibration accuracy in calculating the number of acid reflux events, we used the nadir values of oesophageal pH recorded during the orange juice swallows to determine the accuracy of the calibration of both electrodes in vivo. To define the magnitude of offset adjustment for each system in each individual, we first measured the mean pH of 20 separate samples of orange juice using a bench top laboratory glass pH electrode (Scholar 425 pH meter; Corning Inc., Corning, New York, USA). Holding the temperature at 25°C using a water bath (Precision Water Bath, Winchester, Virginia, USA), we found the pH of orange juice to be 3.88 (SD 0.02). This value was then assumed to be the true pH within the oesophagus during orange juice swallows and was compared with the nadir pH registered by each recording system during the orange juice swallows. The difference between the registered values and 3.88 was then added or subtracted to every data point of the entire 24 hour data set for each electrode, in essence performing a post hoc in vivo calibration at pH 3.88.
Statistical analysis
To determine whether the two systems were in agreement for the detection of reflux events, we divided reflux events into two groups: short and long reflux events. We defined short reflux events as events characterised by 1–3 sequential data points less than pH 4 for the catheter or only 1–2 data point less than pH 4 for the Bravo system. Reflux events were defined as overlapping and simultaneously recorded if a reflux event was noted within 12 seconds of the start or ending of the reflux event of the complementary recording system. This was reported as per cent concordance and was summarised as mean (SD).
Normal data, such as the number of reflux events, were summarised as mean (SD) and compared using the paired Student’s t test. Non-normally distributed data (such as acid exposure time) among subjects were summarised by median values and interquartile range (IQR). Least squares regression analysis was used to determine the correlation between the position of the pH electrode and its effect on the number of reflux events. A p value <0.05 was considered significant.
RESULTS
Detection of acid reflux events (software reported and manual reanalysis)
Complete pH data with in vivo reference measurement from both systems was available for 18 of 25 subjects. One subject did not complete the 24 hour catheter portion secondary to discomfort and two others had irretrievable data because of hardware malfunction (one Digitrapper, one Bravo). In addition, four subjects did not complete the orange juice swallow prior to the initiation of the protocol.
The software reported and manually recalculated number of acid reflux events were significantly greater with the Mark III Digitrapper catheter pH system compared with the Bravo capsule system (table 1 ▶). Each of the 18 subjects had higher values recorded by the Mark III Digitrapper catheter pH system compared with the Bravo capsule system. Analysis to determine whether missing data could account for the apparent difference in number of reflux events between the two systems revealed that this factor had no substantial influence. The average time period during which missing data from the Bravo system overlapped with reflux events recorded by the catheter was less than 60 seconds.
Table 1.
Software reported and manually recalculated number of acid reflux events with the Mark III Digitrapper catheter pH system compared with the Bravo capsule system
| Reflux events per 24 hours | ||
| Catheter | Bravo | |
| Software reported | 117.0 (56.0)* | 41.8 (21.7) |
| Manual recalculation | 112.2 (56.0)* | 40.8 (21.4) |
| Manual recalculation after offset correction | 69.8 (42.3)* | 37.9 (23.4) |
Values are mean (SD).
*p<0.05, catheter versus Bravo.
pH electrode position
Complete electrode position data from 22 subjects could be analysed for day 1; one subject did not tolerate the catheter and the endoclip detached prior to the first measurement in two others. The mean absolute difference in position between the pH electrodes was 1.0 cm (SD 0.87). There was no difference in mean distance between the SCJ and either pH electrode (catheter 7.20 (SD 1.6) cm; Bravo 7.08 (1.38) cm; p>0.5). Complete electrode position data could be analysed for both days in 18 subjects; four additional endoclips detached early. When position data on day 2 were compared with those of day 1, the mean distance from the SCJ to the Slimline catheter pH electrode increased by 7.0 mm (day 1, 7.20; day 2, 7.90; p<0.05). In contrast, the Bravo capsule did not move significantly (day 1, 7.08 cm; day 2, 7.27 cm; p>0.05). The effect of positional separation between the catheter and Bravo pH electrodes on total number of reflux events is illustrated in fig 1 ▶ in which the difference in number of reflux events between the catheter and Bravo capsule is plotted as a function of the spatial separation between the two electrodes. The relationship was not statistically significant (r = 0.01, p>0.05).
Figure 1.

Effect of positional separation of the pH electrodes on the reported number of reflux events (22 subjects, raw data). Position 0 is the location of the Bravo pH electrode. Variations in electrode position within the 4–10 cm range above the squamocolumnar junction domain of the oesophagus did not systematically affect the number of reflux events reported (r = 0.01, p>0.05).
Effect of offset adjustment on number of reflux events
The fact that a systematic offset error existed in recorded pH values was strongly suggested by inspection of the synchronised pH tracings. The magnitude of the offset error varied widely among individuals and between pH recording systems. This is illustrated in fig 2 ▶ in which the nadir pH values obtained during orange juice swallows for 18 individuals are presented for both systems. The mean nadir pH during the orange juice swallows was 3.11 (SD 0.22) for the Slimline catheter and 3.84 (0.02) for the Bravo capsule. Data on electrode drift from beginning to end of the 24 hour study period were available for 12 subjects. The catheter recorded a mean nadir pH of orange juice for the catheter of 2.98 (SD 0.28) at the beginning and 2.93 (0.25) at the end of the study period. Similarly, the Bravo capsule recorded a mean nadir pH of orange juice of 3.71 (0.28) at the beginning and 3.65 (0.21) at the end of the study period.
Figure 2.
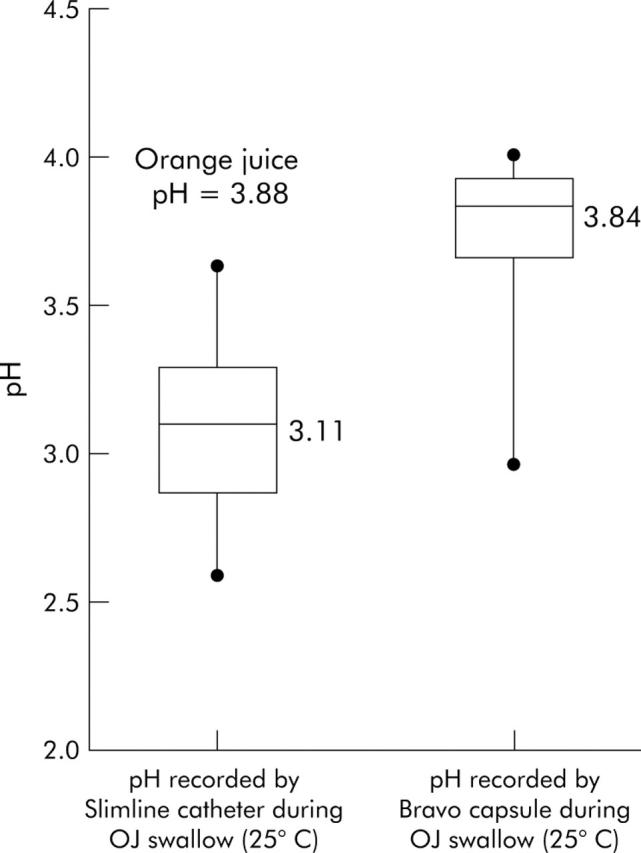
Nadir pH recorded during the orange juice swallow used as a reference pH measurement by the Slimline catheter system and the Bravo pH system. The median nadir pH reference measurement for the Slimline catheter was 3.1 and the nadir pH measurement for the Bravo capsule was 3.8. p<0.05 Slimline versus Bravo.
Applying the offset correction to the 18 subjects in whom this was possible substantially reduced the apparent discrepancy in number of acid reflux events reported by the two systems (table 1 ▶). However, the total number of events was still significantly higher with the Digitrapper system. The effect of offset correction can be further appreciated in fig 3 ▶ in which the total number of reflux events for individual subjects for both systems before and after adjustment are linked.
Figure 3.

Reflux events before and after offset adjustment for both systems for individual subjects. After offset adjustment, the number of reflux events was still significantly different between the two systems but the difference was substantially reduced (table 1 ▶).
Effect of duration of oesophageal acid exposure on reflux event detection
Reasoning that the persistent discrepancy in acid reflux event detection between systems even after offset correction might be attributable to short acid reflux events, we examined the concordance rate between systems for short and long events. Doing so, we found that the number of short events recorded by the catheter system was more than twice that recorded by the Bravo system while long events were recorded in similar numbers between the two systems (fig 4 ▶). In addition, short events were less likely to be recorded simultaneously by the two systems, as evident by the low concordance rates shown in table 2 ▶. On the other hand, the two systems had much higher concordance for longer acid reflux events (table 2 ▶). Our rationale for distinguishing short reflux events from longer ones is evident in fig 5 ▶. Very brief reflux events were often characterised by minor fluctuations above and below the threshold value of pH 4 whereas longer reflux events were typically associated with a lower nadir pH, and consequently greater values of integrated oesophageal acidity.
Figure 4.

Number of reflux events per 24 hours segregated into short events and long events. The discrepancy in number of reflux events detected between systems was most pronounced in the shorter events of which the catheter detected more than twice the number detected by the Bravo system. Of note, a substantial proportion of short events had nadir pH values greater than 3.8, suggesting minimal acid burden.
Table 2.
Breakdown of reflux event tally based on whether events were short (one or two data points for the catheter system or only one for the bravo system) or long
| Slimline catheter | Bravo | |||
| Short events | Long events | Short events | Long events | |
| No of events/24 h (mean (SD)) | 45.5 (25.5)*† | 24.3 (18.6) | 18.5 (9.5) | 19.4 (14.9) |
| Concordance with Bravo (%) | 32.7 | 76.8 | – | – |
| Concordance with catheter (%) | – | – | 49.3 | 93.5 |
| Nadir pH of events (mean (SD)) | 3.1 (0.2)*† | 2.8 (0.4)* | 3.5 (0.3)† | 3.1 (0.3) |
| Total integrated acidity, all subjects (mmol min/l) | 162.1 | 1986.8 | 15.0 | 1430.1 |
*p<0.05, catheter versus Bravo similar reflux event duration; †p<0.05, short versus long within pH system (catheter or Bravo).
Figure 5.

Simultaneous tracings from the catheter and Bravo system illustrating an example of discrepant detection of short acid reflux events (one or two data points for the catheter and only one data point for the Bravo system). During a five minute epoch, multiple short reflux events with minor fluctuation around the threshold value of pH 4 are evident even after the pH offset adjustment for the catheter. These events are not significant in the context of integrated oesophageal acidity and likely represent false reflux events due to artefact or movement of the catheter relative to the mucosa. In contrast, the longer reflux event is associated with a lower nadir pH, and consequently concordance between electrodes and greater values of integrated oesophageal acidity.
The impact of the discrepancy in the number of reported short reflux events on the overall oesophageal acid exposure measured by the two recording systems was minimal. In fact, after pH offset adjustment, the median acid exposure time for the two systems was statistically similar despite the large discrepancy in the number of reflux events reported (Digitrapper 0.90% (IQR1.33%); Bravo 1.16% (IQR 2.33%)). Other ways of analysing the impact of these short events was to calculate the nadir pH associated with them or to compute the associated integrated oesophageal acidity. These tabulations are shown in table 2 ▶ and fig 6 ▶, categorising reflux events as short or long. Evident from the analysis, the overall impact of short events on oesophageal acid exposure or oesophageal acid burden was substantially less than that of long events despite long events being substantially less frequent.
Figure 6.

Mean integrated oesophageal acidity (IOA) of the reflux events of each individual was calculated and revealed that short acid reflux events were associated with minimal acidity. The cumulative totals of all subjects revealed that, despite having many more events, the short reflux events did not contribute substantially to overall oesophageal acid burden.
DISCUSSION
This study assessed two ambulatory oesophageal pH monitoring systems with respect to acid reflux event detection during simultaneous recordings in 25 asymptomatic subjects. The respective datasets were then compared to ascertain the degree of discrepancy and the reasons for discrepancy between systems. The major findings were that the Slimline catheter based Mark III Digitrapper pH system typically reported almost three times the number of acid events reported by the wireless Bravo system. Of these, 40% of the excess events were attributable to electrode calibration inaccuracy, evident from the in vivo measurement of orange juice of predetermined pH. Most of the remaining excess events were of 1–3 data points (1–17 s) and associated with negligible intraoesophageal acidity.
Although this study is not the first to directly compare the Bravo wireless system with a conventional catheter system, it is the first to focus predominantly on acid reflux event detection. Prior studies looking to validate the wireless Bravo system focused on the oesophageal acid exposure time.3–5 Hakansson studied 30 subjects and found acid exposure values with the catheter system to be 1.5% greater (30% in relative terms) than with the Bravo system3; Bruley des Varannes and colleagues found acid exposure values with the catheter system to be 1.2% greater than with the Bravo system.4 On initial inspection of our raw data, we also found a difference of similar magnitude (1.6%) between the two recording systems.5 In the process of data analysis we found that the most overt abnormality noted was a consistent offset in pH values recorded by the two systems. This was corroborated by our in vivo reference measurement using swallowed orange juice, revealing that the Slimline catheter system consistently measured a pH value of 0.77 pH units less than our ex vivo reference measurement of pH 3.88 while the Bravo was minimally offset (fig 2 ▶).
In the current study, analysing the detection of acid reflux events, we once again hypothesised that the same issue of offset correction would likely contribute to any observed discrepancy between systems in the reported number of acid reflux events. Although this adjustment did reduce the observed discrepancy by approximately 40%, the catheter system on average still recorded almost twice as many acid reflux events as the Bravo system. We then explored other hypotheses that could be responsible for this observed discrepancy. Missing data points were minimal and responsible for negligible discrepancy. Another potential source of discrepancy was the lesser sampling rate of the Bravo system. To estimate the potential impact of the 10 per minute versus 15 per minute sampling rates, we applied data from an elegant analysis done by Emde and colleagues.7 These investigators used an ultrafrequent pH recording system (256 samples per minute) to original data sets of pH recordings and then successively halved the sampling rate to ascertain the effect on event detection. They found no decrement in event detection as the sampling rate was reduced to one per second, suggesting this to be optimal, but then a progressive decrease in event detection with lesser sampling rates. A sampling rate of 16 per minute, similar to the every fourth second rate used for Slimline would miss approximately 30% of all reflux events while a sampling rate of eight per minute, close to the every sixth second interval used for the Bravo system, would miss 37% of all reflux events. Thus although both systems will miss a substantial number of brief events, the increased detection attributable to increasing the sampling rate from every sixth second to every fourth second would likely be of the order of 10%.
Given previous data demonstrating that reflux event detection increases with the proximity of the pH electrode to the SCJ,8,9 we analysed the electrode positioning data as a determinant of reflux event detection. In contrast with previous data using the same type of pH monitoring system in the same individual, we found no systematic relationship between which electrode (Slimline or Bravo) was closer to the SCJ and which detected the greater number of acid reflux events. In fact, we concluded that variations in electrode position within the domain 4 –10 cm proximal to the SCJ using the two different pH monitoring systems did not substantially affect the number of acid reflux events detected (fig 1 ▶). This is also supported by the observation that there was no significant difference in the mean placement position above the SCJ between the Slimline catheter electrode and the Bravo capsule.
With no overt technical or methodological explanations for the persistent discrepancy in the number of reflux events reported by the two systems, we altered our focus to ascertain the characteristics of the discordant reflux events. As many events reported by the Slimline catheter system were of very brief duration, we separated events into short events (1–3 data points for the catheter and 1–2 for the Bravo capsule) and long events (at least four consecutive data points for the catheter and three or more for the Bravo capsule). We found that the majority of discordance was with short events. Furthermore, there was poor concordance between systems in recording short events while concordance for longer events was very good. Although the aetiology of this discordance was not explained by our protocol, we hypothesise that the low sampling rates of both systems coupled with the frequent occurrence of brief periods of acid exposure may explain a major part of the discrepancy. The Bravo system theoretically should detect all events greater than or equal to six seconds while the Slimline system should detect all events equal to or greater than four seconds. However, both systems will fail to detect increasing numbers of events as those events are progressively briefer than the system sampling rates. Furthermore, because the instant of sampling is not synchronised between systems, the two systems will capture (and miss) different events. Ultimately, our study is limited in its ability to analyse this effect as we do not have a sample rate of 60 per minute for comparison.
The above findings, namely that the detection of very brief reflux events is inconsistent, argues that the significance of such events should be reconsidered. In terms of overall acid exposure, be it quantified in time or intraoesophageal acidity, our findings clearly demonstrate that these short events are a very minor contributor, collectively accounting for less than 8% of the overall cumulative integrated acidity measured. Whether or not these short acid reflux events are important in generating symptoms is unknown but it is reasonable to suspect that they have less clinical relevance with respect to acid mediated symptoms than longer events that are characterised by lower nadir pH and substantially greater intraoesophageal acidity. Coupling this observation with the unreliable detection of these short events, one can speculate that symptom association schemes are weakened by their inclusion. At the very least, work on symptom association indices needs to be redone for the Bravo system in the face of vastly reduced numbers of acid reflux events reported.
In summary, we found substantial discrepancy in reflux event detection between the Slimline catheter based Mark III Digitrapper pH system and the wireless Bravo system. Forty per cent of this discrepancy was attributable to electrode inaccuracy. The remainder of the discrepancy was mainly attributable to very brief (1–17 s) reflux events. Although we could not explain the exact aetiology of these brief events, we suspect that many arise from the low (and different) sampling rates of the two systems and the effect of movement of the catheter relative to the mucosa during swallowing or respiration. Further studies combining impedance with pH monitoring will likely be useful in determining the relevance of these short events in eliciting symptoms.10 We conclude that future analyses of acid reflux-symptom correlation using pH monitoring systems would likely demonstrate a stronger association by utilising an in vivo method of pH calibration and restricting the analysis to longer events, evident by three or four sequential subthreshold pH measurements.
Acknowledgments
This work was supported by RO1 DC00646 (PJK) and K23 DK062170-01 (JEP) from the Public Health Service as well as an unrestricted grant and contributed devices from Medtronic Inc., Shoreview, MN, USA.
Abbreviations
SCJ, squamocolumnar junction
LOS, lower oesophageal sphincter
GORD, gastro-oesophageal reflux disease
IQR, interquartile range
Published online first 28 May 2005
Conflict of interest: None declared.
REFERENCES
- 1.Johnsson F, Joelsson B. Reproducibility of ambulatory oesophageal pH monitoring. Gut 1988;29:886–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Murphy DW, Yuan Y, Castell DO. Does the intraesophageal pH probe accurately detect acid reflux? Simultaneous recording with two pH probes in humans. Dig Dis Sci 1989;34:649–56. [DOI] [PubMed] [Google Scholar]
- 3.Hakansson G. Swedish Surgical Week. Stockholm, 16–20 August 2004.
- 4.Bruley des Varannes S, Mion F, Ducrotte P, et al. Simultaneous recordings of esophageal acid exposure using conventional pH monitoring and the Bravo telemetric catheter free system: analysis of concordance. Gastroenterology 2004;126:A318. [Google Scholar]
- 5.Pandolfino JE, Shi G, Lee TJ, et al. Comparison of endoscopic placement of the Bravo pH capsule and a conventioanl pH catheter using manometric landmarks. American Motility Society. Rochester, Minnesota, September 2004.
- 6.Pandolfino JE, Richter JE, Ours T, et al. Ambulatory esophageal pH monitoring using a wireless system. Am J Gastroenterol 2003;98:740–9. [DOI] [PubMed] [Google Scholar]
- 7.Emde C, Garner A, Blum AL. Technical aspects of intraluminal pH-metry in man: current status and recommendations. Gut 1987;28:1177–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Weusten BL, Akkermans LM, vanBerge-Henegouwen GP, et al. Spatiotemporal characteristics of physiological gastroesophageal reflux. Am J Physiol 1994;266:G357–62. [DOI] [PubMed] [Google Scholar]
- 9.Fletcher J, Wirz A, Henry E, et al. Studies of acid exposure immediately above the gastro-oesophageal squamocolumnar junction: evidence of short segment reflux. Gut 2004;53:168–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sifrim D, Castell D, Dent J, et al. Gastro-oesophageal reflux monitoring: review and consensus report on detection and definitions of acid, non-acid, and gas reflux. Gut 2004;53:1024–31. [DOI] [PMC free article] [PubMed] [Google Scholar]