

Abstract
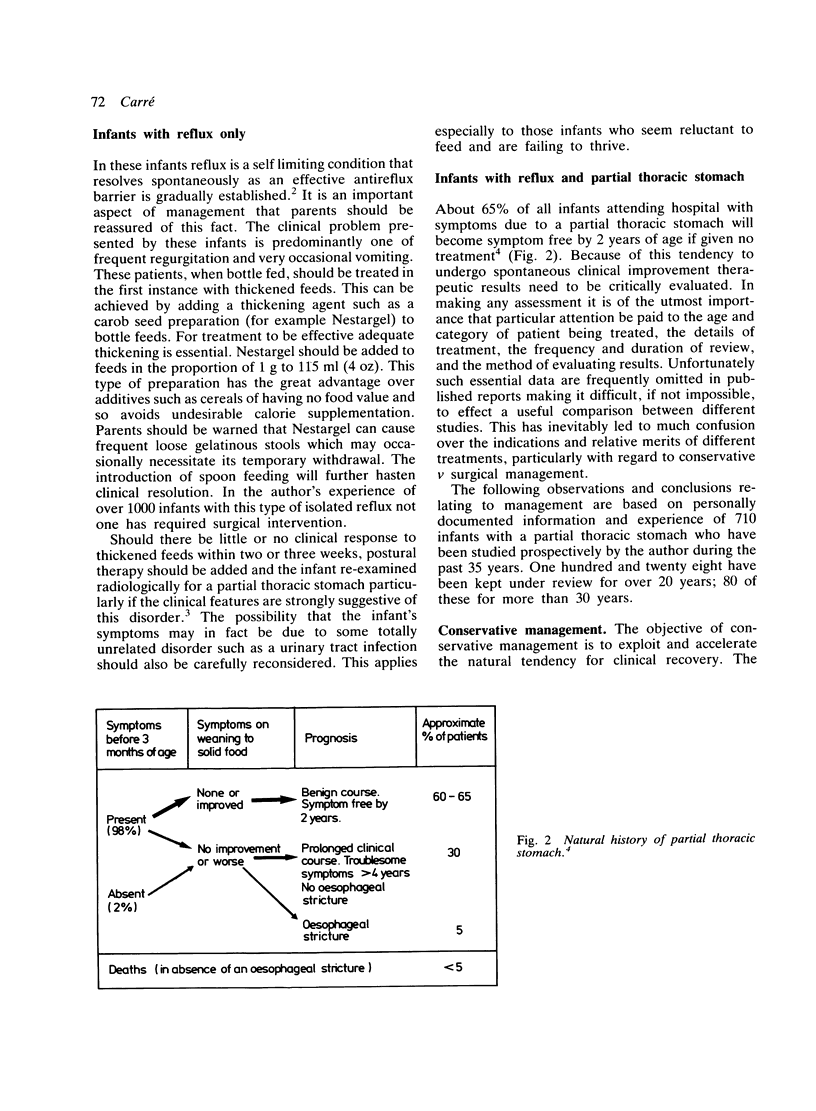
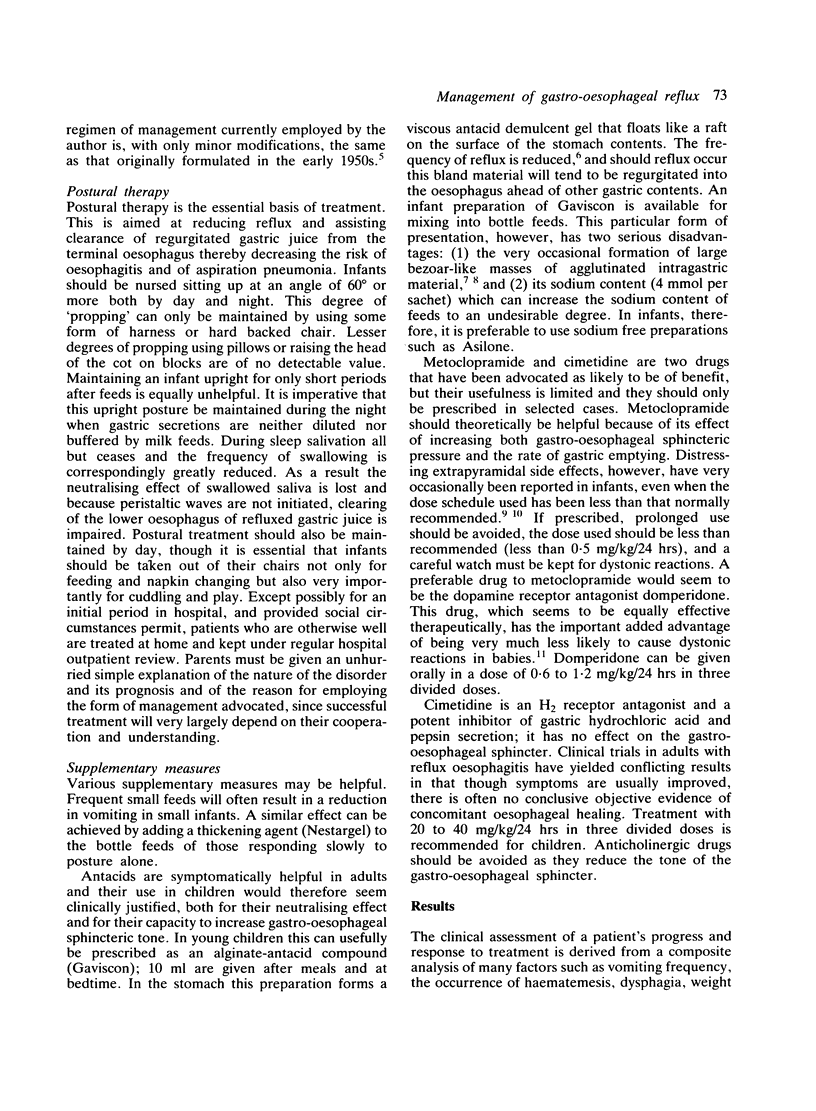
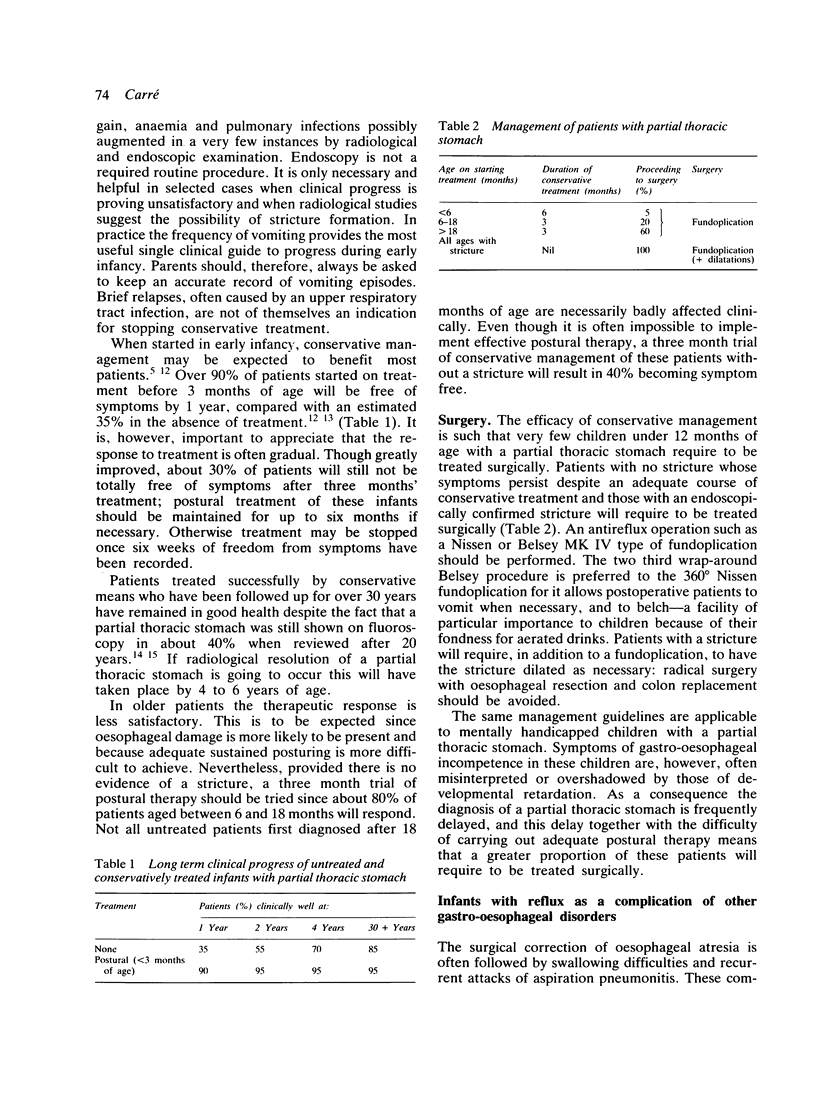
Parental reassurance and thickened feeds are the only requirements in the management of infants with reflux when this is the sole detectable gastro-oesophageal abnormality. In view of the strong propensity for spontaneous clinical resolution and the excellent results achieved by conservative management, infants with reflux due to a partial thoracic stomach (hiatal hernia) uncomplicated by a stricture should be treated in the first instance by postural therapy, with or without thickened feeds and supplements of antacids, domperidone, and cimetidine. Those showing no response after an adequate period of conservative treatment should have an antireflux operation. The Belsey MK IV type of fundoplication is preferred. Only an exceptional patient will require to be treated surgically before 12 months of age. The same surgical antireflux procedure, combined with oesophageal dilatations as necessary, is the treatment of choice for patients with a partial thoracic stomach complicated by a reflux oesophageal stricture. A similar treatment regimen should be followed for patients with reflux after repair of an oesophageal atresia. Surgical correction is mandatory for all infants with reflux due to a large combined hiatal hernia.
Full text
PDF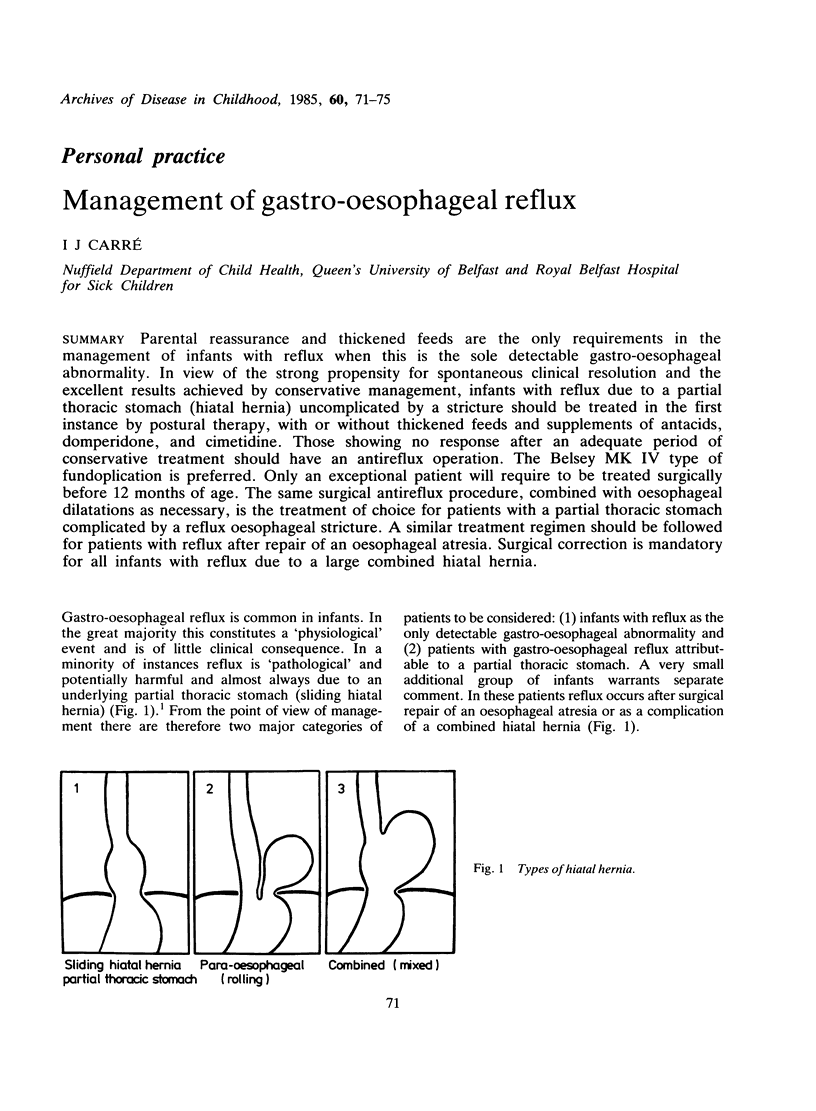

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Boix-Ochoa J., Canals J. Maturation of the lower esophagus. J Pediatr Surg. 1976 Oct;11(5):749–756. doi: 10.1016/0022-3468(76)90099-3. [DOI] [PubMed] [Google Scholar]
- CARRE I. J. Postural treatment of children with a partial thoracic stomach ('hiatus hernia'). Arch Dis Child. 1960 Dec;35:569–580. doi: 10.1136/adc.35.184.569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- CARRE I. J. The natural history of the partial thoracic stomach (hiatus hernia) in children. Arch Dis Child. 1959 Aug;34:344–353. doi: 10.1136/adc.34.176.344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Low L. C., Goel K. M. Metoclopramide poisoning in children. Arch Dis Child. 1980 Apr;55(4):310–312. doi: 10.1136/adc.55.4.310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pieretti R., Shandling B., Stephens C. A. Resistant esophageal stenosis associated with reflux after repair of esophageal atresia: a therapeutic approach. J Pediatr Surg. 1974 Jun;9(3):355–357. doi: 10.1016/s0022-3468(74)80292-7. [DOI] [PubMed] [Google Scholar]
- Reid M. Dystonic reactions to metoclopramide (maxolon). Ulster Med J. 1977;46(1):38–40. [PMC free article] [PubMed] [Google Scholar]